Abstract
Performance of the Ponto Plus bone-anchored sound processor from Oticon Medical was evaluated in 19 subjects relative to its predecessor, the Ponto Pro. All subjects had mixed and conductive hearing loss with ample experience with bone-anchored hearing devices. Sixteen subjects were fitted on one side and three subjects on both sides.
One of the new features in Ponto Plus is a link to a body-worn ‘streamer’ for wireless connectivity. The efficacy of wireless signal transfer was tested with speech-in-noise measures. When setting equal wireless and microphone output levels, speech scores were essentially similar, thus confirming the equivalence of both input modes.
To simulate real-life conditions, streamer output is usually +6 dB or +9 dB higher than microphone output depending on the type of streamer input. For our target group, this streamer advantage directly translates into more favourable signal-to-noise ratios in difficult listening conditions. The real-life benefit of wireless signal routing with the telephone or when listening to TV was evaluated with a proprietary questionnaire. The scores on speech quality, speech-in-quiet and speech-in-noise were significantly higher (p<1%) for Ponto Plus than for Ponto Pro. The annoyance of ambient noise was significantly lower (p<5%) for Ponto Plus than for Ponto Pro.
Another difference between Ponto Plus and Ponto Pro is an increase in mid- and high-frequency output of about 4.5 dB for Ponto Plus relative to Ponto Pro. This increase resulted in a significantly (p<5%) higher average score for the speech quality domain of the Speech, Spatial, and Qualities of Hearing (SSQ) questionnaire of Gatehouse and Noble (2004) for Ponto Plus. For microphone input, speech reception thresholds in noise were about equal for Ponto Plus and Ponto Pro.
Proprietary questionnaires showed a (strong) preference for Ponto Plus with streamer over Ponto Pro in 13 out of 19 subjects, thus underlining the importance of wireless connectivity. In fact, they regarded wireless connectivity the most important distinction between Ponto Plus and Ponto Pro.
Introduction
For individuals with conductive or mixed hearing loss needing amplification who cannot use a conventional hearing aid due to draining ears or atresia of the ear canal, for example, a bone-anchored hearing device (BAHD) is a well-known option. A BAHD consists of a titanium implant anchored in the mastoid, a skin-penetrating abutment, and a sound processor. The sound processor transforms sound into mechanical vibrations that are transmitted through the abutment and implant to the skull. This direct transmission of mechanical energy is 10 to 15 dB more efficient than sound transmission via skin and underlying tissues with conventional bone conduction (Håkansson, Tjellström, & Rosenhall, 1984; Verstraeten, Zarowski, Somers, Riff, & Offeciers, 2009).
Users of BAHDs generally do well in quiet, but they often experience difficulties when faced with more challenging listening conditions, such as communicating in noise and using the telephone. Some of these difficulties may be alleviated with wireless technology. The recently released Ponto Plus sound processor from Oticon Medical features wireless connectivity with a body-worn ‘streamer’ linked to the sound processor. The streamer enables wireless connections to mobile phone, landline phone, radio and TV, to an external microphone, and to other Bluetooth-based audio devices.
The aim of this study is to assess the additional value of the Ponto Plus sound processor with streamer relative to the Ponto Pro sound processor, also from Oticon Medical. The main focus of this paper is on assessing the benefits of wireless connectivity. Secondly, as the Ponto Plus provides more output at mid- and high frequencies than Ponto Pro the microphone performance of both devices will be evaluated in a sound-field setting. Both devices will be evaluated in 19 subjects having ample experience with BAHDs.
Methods
The outputs of Ponto Pro and Ponto Plus were measured on a TU-1000 skull simulator (Håkansson & Carlsson, 1989) with ICRA noise presented at 47, 62, and 77 dB SPL (Dreschler, Verschuure, Ludvigsen, & Westermann, 2001).
The average frequency response for the devices of the first 13 subjects is shown in Figure 1 for Ponto Plus (blue curve) and for Ponto Pro (red curve). Both devices were programmed in user settings. Figure 1 shows that the resonance frequency for Ponto Plus is slightly higher than for Ponto Pro, but more importantly, the output of Ponto Plus appears to be about 4.5 dB higher for frequencies above 2 kHz. Note that the skull simulator does not fully reflect the patient’s response for frequencies around the resonance frequency. When applying both devices on an abutment with real patients the differences in resonance frequency disappear, but the increased output for Ponto Plus for frequencies above 2 kHz remains.
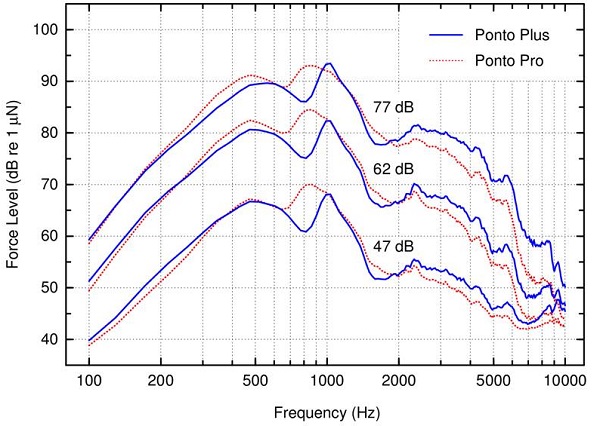
Figure 1. Frequency response of the Ponto Pro and Ponto Plus sound processors on a TU-1000 skull simulator (Håkansson & Carlsson, 1989). The stimulus consisted of ICRA noise (Dreschler, et al., 2001; two person babble, 1 male, 1 female) at 47, 62, and 77 dB SPL. ICRA noise was selected for its speech-like temporal and spectral properties. The TU-1000 was positioned in an acoustically treated box (Interacoustics TBS-25) and its output was analysed with an Interacoustics Equinox running HIT 440 2.0.4. SP2 software.
Twenty patients were included in the study on the basis of hearing configuration, BAHD experiences and (most) bone conduction thresholds within the fitting range of a standard BAHD device (Snik, Mylanus, Proops, Wolfaardt, Hodgetts, et al., 2005). One patient was excluded from the study on the basis of bone conduction thresholds that were well outside this fitting range. She opted for a more powerful bone-anchored device (Bosman, Snik, Mylanus, & Cremers, et al., 2013).
All 19 patients, with ages ranging from 26 to 73 years (average: 46.1 years) had a bilateral conductive or mixed hearing loss. Patient thresholds were measured with standard procedures and equipment (Interacoustic Equinox audiometer fitted with TDH39 headphones and B-71 bone conductor). The average air and bone conduction thresholds together with their standard deviations are shown in Figure 2. The average air and bone conduction thresholds at 0.5, 1, 2, and 4 kHz were 57.0 dB and 15.4 dB for the left side and 65.7 dB and 18.2 dB for the right side, respectively.
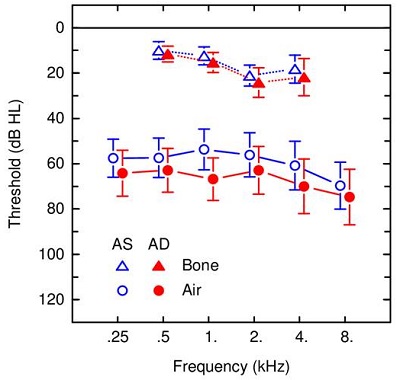
Figure 2. Average pure-tone thresholds with interindividual standard deviations for 19 subjects. Air conduction thresholds are shown with circles and bone conduction thresholds with triangles. Data for the left side are shown in blue and for the right side in red.
In four patients the loss was due to chronic suppurative otitis media, in eight to a radical mastoidectomy, and in five to bilateral congenital atresia. Fourteen patients had experience with a Ponto Pro. Four patients had a Cochlear Baha Divino, and one patient had a Cochlear Baha Compact. These latter five patients were given a 6-week acclimatization period with Ponto Pro before entering the study. Sixteen patients were fitted on one side and three patients on both sides.
Speech perception in noise was measured with Plomp and Mimpen (1979) sentences against a background of filtered noise with the same long-term average spectrum of the speaker (long-term average speech spectrum, LTASS, noise). The sentences containing 8 or 9-syllables are representative of everyday Dutch. The Speech Reception Threshold (SRT) for sentences was measured by varying the speech level with a ‘one step up, one step down’ procedure. Speech was presented frontally at 0° azimuth with 65-dBA masking noise either at 0° or 90° azimuth (S0N0 or S0N90 condition) at the ipsilateral, implanted side. Both Ponto Pro and Ponto Plus were tested in omni-directional mode and in ‘full-focus’ directional mode. Subjective evaluations were carried out with the SSQ questionnaire (Gatehouse & Noble, 2004) and proprietary questionnaires.
Results
Figure 3 shows the results for sentence perception in noise for Ponto Pro and Ponto Plus in the S0N0 condition in omni-directional mode and in the S0N90 condition in both omni-directional and in directional mode. There are no statistically significant differences (p>5%) between both devices. In the S0N0 condition, an SRT of -3.7 dB signal-to-noise ratio was found. The reference value in this condition for normal-hearing subjects is -5.4 dB (Plomp & Mimpen, 1979). Moving the noise source from 0° to 90° azimuth increases the SRT by 1.3 dB. With both devices set to full-focus directionality, the SRT in the S0N90 condition improves (is lowered) by 1.8 dB to -4.1 dB, closely to the value for the S0N0 condition. Apparently, the additional gain for mid and high frequencies for the Ponto Plus relative to the Ponto Pro has no statistically significant effect (p>5%) on speech perception in noise.
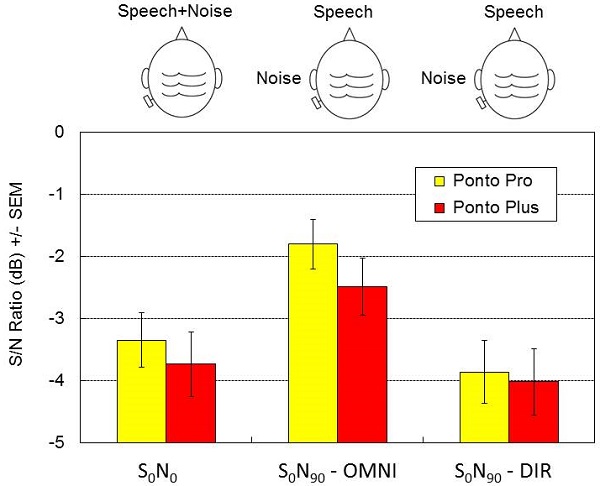
Figure 3. Speech-in-noise results in sound field for Ponto Pro and Ponto Plus. Speech was presented at the front and the masking noise either at the front (S0N0) or at the BAHD side (S0N90). Results for the S0N90-condition are shown for omni-directional (S0N90 - OMNI) and full directional microphone (S0N90 - DIR) mode. Differences between the two devices were not statistically significant (p>0.05).
In the subjective evaluation of Ponto Plus and Ponto Pro with the SSQ questionnaire (Gatehouse & Noble, 2004), scores for the Quality domain were significantly higher (p<5%) for the Ponto Plus than for Ponto Pro (Figure 4). Differences for the Speech and Spatial domains failed to reach statistical significance (p>5%).
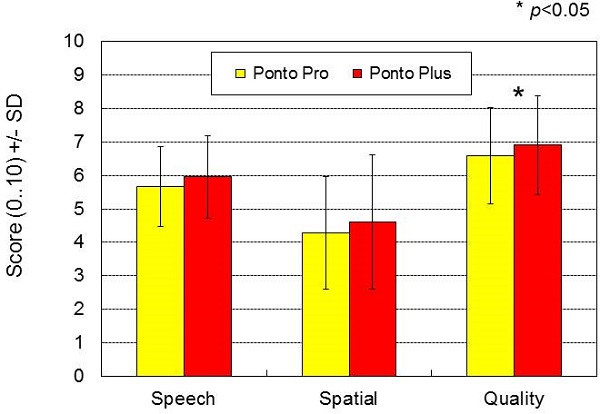
Figure 4. Results for the Speech, Spatial and Quality of hearing questionnaire (Gatehouse & Noble, 2004) for Ponto Pro and Ponto Plus. The difference between the two devices was only statistically significant for the Quality domain (p<0.05).
The results on proprietary questionnaires using visual-analogue scales probing speech quality, speech intelligibility in quiet and noise, and annoyance by ambient noise when using the telephone are shown in Figure 5. The visual-analogue scales ranged for the speech quality and intelligibility questions from extremely poor to excellent and for the annoyance by ambient noise from very annoyed to not at all annoyed. Seven subjects completed the questionnaire for landline phone and nine subjects for mobile phone. Figure 5 shows a substantial and highly significant positive effect (p<0.01) of streamer input versus microphone input for the telephone. Annoyance by ambient noise is statistically significant at p<0.05, due to a smaller number of respondents, especially for landline phone.
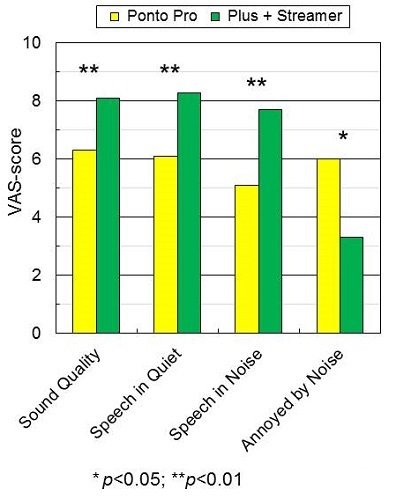
Figure 5. Visual-analogue-scores for Ponto Pro and Ponto Plus with streamer for telephone (landline telephone: 7 subjects; mobile phone: 9 subjects). Scores for speech quality, speech in quiet, and speech in noise were significantly higher for Ponto Plus with streamer than for Ponto Pro (p<0.01). The annoyance by ambient noise was significantly lower for Ponto Plus with streamer than for Ponto Pro (p<0.05).
Questions regarding TV were answered by 15 subjects (Figure 6). Again, all differences between microphone and streamer input are large and statistically significant (p<1%).
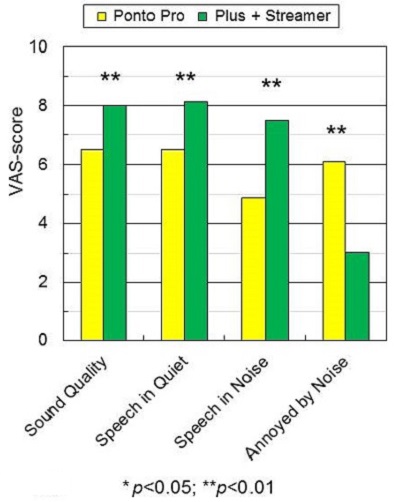
Figure 6. Visual-analogue-scores for television. Scores for speech quality, speech in quiet, and speech in noise were significantly higher for Ponto Plus with streamer than for Ponto Pro (p<0.01) and the annoyance by ambient noise was significantly lower for Ponto Plus with streamer than for Ponto Pro (p<0.01).
Figure 7 shows the results for the overall question on device preference. Thirteen participants prefer Ponto Plus with streamer over Ponto Pro. Figure 8 shows that for 11 out of 13 participants this preference is partly based upon the additional functionality offered by the streamer.
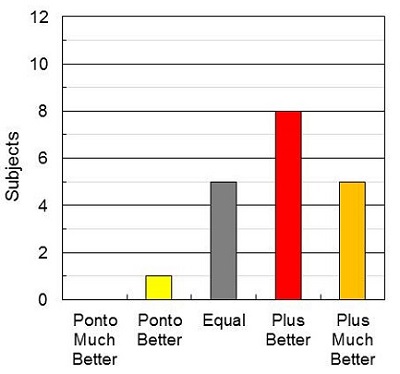
Figure 7. Thirteen subjects preferred the Ponto Plus with streamer over the Ponto Pro.
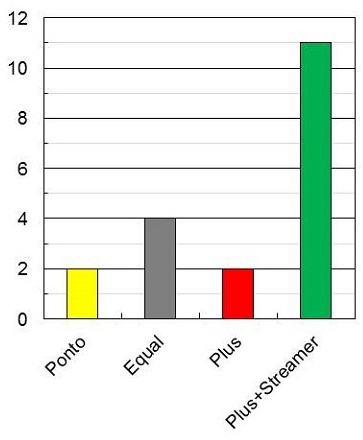
Figure 8. Eleven out of the thirteen subjects who preferred the Ponto Plus with streamer based their preference for Ponto Plus on streamer functionality.
Discussion
The most prominent findings of this study are the equivalent scores for microphone and streamer input for carefully matched output levels. The equivalence of microphone and streamer input essentially corroborates the viability of a streamer for high-quality signal transfer. For practical applications, this finding is highly relevant, as (mobile) telephone wireless connectivity implies a release from the burden of searching for an optimal position of telephone receiver and sound processor while balancing feedback issues. In fact, with a streamer providing wireless connectivity, the exact position of telephone and sound processor becomes largely irrelevant.
A major advantage of wireless signal routing is that under unfavourable listening conditions it can provide signals with a much better signal-to-noise ratio to the listener than the BAHD microphone(s). This is especially true for (mobile) telephone, TV, and other applications allowing for direct transmission of the source signal to the hearing device. In fact, for some patients, this was the first time they could use their mobile phone with its built-in loudspeaker.
In conductive and mixed hearing loss, sound entering the ear canal is attenuated by the conductive component (‘air-bone gap’) of the loss, making this an ideal target group to benefit from wireless signal routing. The ratio of streamer and microphone output may be easily set to the listeners’ preference with little interference from direct, unamplified sound. For example, the American Speech-Language-Hearing Association’s (ASHA; 2002) guideline for FM systems requiring a 10-dB higher output for streamer output relative to an equivalent microphone input may thus be easily realised. Note that the output levels for microphone and streamer inputs and the spectral balance for streamer input can be set individually with the Genie Medical fitting software and separately for the different streamer input types.
In practice, many subjects appreciated streamer input, especially in conditions with ambient noise. During the experiments, a TV demo-setup running news items has been instrumental in realising acceptance of the streamer input with Ponto Plus. For this setup, subjects almost instantaneously mentioned better speech intelligibility and reduced listening effort.
In our experiments, the increase in mid- and high-frequency output with Ponto Plus had little effect on speech intelligibility in sound field as both speech and the LTASS masking noise were presented well above threshold for both devices. However, these spectral differences did have a statistically significant effect on the scores for the sound quality domain of the SSQ questionnaire (p<5%).
In conclusion, this study shows equivalent speech intelligibility for streamer and microphone signals when calibrated for equal output levels. Ponto Plus provides more high-frequency output than Ponto Pro leading to significant better ratings for the sound quality of the SSQ, but without significant differences in speech intelligibility scores. Using the default output levels for streamer and microphone signals resulted for most subjects in a strong preference for the combination of microphone input and wireless connectivity.
References
American Speech-Language-Hearing Association. (2002). Guidelines for fitting and monitoring FM systems. Retreived from www.asha.org/policy/GL2002-00010.htm
Bosman, A. J., Snik, A. F. M., Mylanus, E. A. M., & Cremers, C. W. R. J. (2013). Evaluation of a new powerful bone-anchored hearing system - a comparison study. Journal of the American Academy of Audiology, 24, 505-513.
Dreschler, W. A., Verschuure, H., Ludvigsen, C., & Westermann, S. (2001). ICRA noises: Artificial noise signals with speech-like spectral and temporal properties for hearing instrument assessment. Audiology, 40(3), 148–157.
Gatehouse, S., & Noble, W. (2004). The Speech, Spatial and Qualities of Hearing Scale (SSQ). International Journal of Audiology, 43, 85-99.
Håkansson, B., Tjellström, A., & Rosenhall, U. (1984). Hearing thresholds with direct bone conduction versus conventional bone conduction. Scandinavian Audiology, 13, 3-13.
Håkansson, B., & Carlsson, P. (1989). Skull simulator for direct bone conduction hearing devices. Scandinavian Audiology, 18(2), 91–98.
Plomp, R., & Mimpen, A. M. (1979). Improving the reliability of testing the speech reception threshold for sentences. Audiology, 18, 43-52.
Snik, A. F., Mylanus, E. A., Proops, D. W., Wolfaardt, J. F., Hodgetts, W. E., et al. (2005). Consensus statements on the BAHA system: Where do we stand at present? Annals of Otology, Rhinology & Laryngology Supplement, 195, 2–12.
Verstraeten, N., Zarowski, A. J., Somers, T., Riff, D., & Offeciers, E. F. (2009). Comparison of the audiologic results obtained with the bone-anchored hearing aid attached to the headband, the testband, and to the ‘snap’ abutment. Otology & Neurotology, 30(1), 70–75.
Cite this content as:
Bosman, A., Snik, A.F.M., & Mylanus, E.A. (2014, May). Evaluating Oticon Medical Ponto Plus and Ponto Plus Sound Processor. AudiologyOnline, Article 12616. Retrieved from: https://www.audiologyonline.com


