
This text course is an edited transcript of an Oticon Medical webinar on AudiologyOnline.
Learning Outcomes
After this course, participants will be able to:
- Describe when the MIPS surgical procedure is appropriate.
- Describe patient indications.
- Discuss the importance of the speech envelope on speech intelligibility.
- Describe the newly FDA cleared abutment extender.
Introduction and Overview
Along with Oticon, Oticon Medical is part of the William Demant family of companies. Oticon Medical’s core business is hearing implant solutions, which includes Ponto bone anchored hearing systems. Our driving force is about putting people first -- putting the patient in the center of everything we do. We strive to deliver life-long patient outcomes based on innovative solutions and support.
Today, I will begin with the fundamentals of bone anchored technology including an overview of osseointegration, and that will give us the foundation to discuss patient candidacy as well as surgical and fitting considerations. I will review Ponto practicalities, such as how the processor was designed to be durable and reliable – which is especially important when we fit children. I will talk about the signal processing in the Ponto processors and present evidence that supports how it benefits our youngest bone anchored patients.
When fitting children with amplification, what is the goal? Parents typically ask us, "Will my child be able to hear? Will they be able to talk? Will they be able to achieve the same things that their brothers and sisters or other children can achieve?"
Parents want to know what it takes for their child to have the most success at school. Is there a technology that will make it easier for them, especially as they get older and academics become harder and harder? As audiologists, these are our goals too. It is important to know that the solutions you offer are the right ones to help each child hear and talk and succeed. After today's course, I also hope you leave with the knowledge that Ponto systems help you meet the needs and the goals of the children and the families that you serve. We believe at Oticon Medical that sound matters, and that children with hearing loss should have access not just to sound, but to a superior sound experience, so that they can achieve the highest degree possible.
The Fundamentals of Bone Conduction and Osseointegration
Bone anchored hearing systems are designed to use the body's natural ability to transfer sound through bone conduction. Sounds are converted to vibrations, which the skull transmits directly to the inner ears.
A Ponto bone anchored hearing system consists of three parts (Figure 1):
- A small (3 or 4 mm) titanium implant that is surgically implanted into the bone behind the ear.
- An abutment that is seamlessly placed through the skin enabling the sound processor to be attached.
- A sound processor that clicks easily to the abutment and sits discreetly behind the ear.

Figure 1. Three components of a Ponto bone anchored hearing system.
The important factor by which osseointegration is achieved is a biocompatibility of living bone with titanium metal. Osseointegration is the foundation for bone anchored devices. By definition, it is the formation of a direct interface between an implant and bone. Bone grows into the grooves of the implant right up to the implant's surface without involvement of the soft tissue layer. No scar tissue, and no cartilage or ligament fibers are present between the bone and the implant surface. The image you see here is of actual osseointegration with titanium (Figure 2).

Figure 2. Living bone tissue integrating with Titanium.
When the Ponto processor is clicked onto the abutment, it picks up sound much the same way a conventional hearing aid does. However, instead of sending sound waves through the ear canal to the middle ear, it transforms them into sound vibrations. This approach -- a direct connection between the sound processor and the bone through the implant abutment -- provides the clearest sound with the most output and gain. A direct drive system like this provides for maximum audibility in the high frequency region. We know how important this is for the development of speech and language, as well as understanding in complex environments. Sometimes we forget that children are in very complex listening environments. Later, I will present evidence to support the benefits of access to high frequency information, especially in very young patients.
Patient Indications and Candidacy
Who can benefit from a bone anchored system? The Ponto system, and bone anchored technology in general, is intended for patients with conductive and mixed hearing loss, as well as patients with single-sided deafness (SSD).
Conductive and Mixed Hearing Loss
These children benefit by having the sound signal bypass the conductive element of their hearing loss and stimulate the inner ears. These are children who have malformations of the outer ear, such as Atresia/Microtia, and/or various cranial-facial syndromes such as Treacher Collins, Goldenhar and CHARGE syndromes. It can also include children with ear canal and middle ear problems, such as Chronic Otitis Media. The hearing loss could be unilateral or bilateral.
When we look at the audiogram for conductive and mixed losses, look at the bone conduction thresholds at 500, 1000, 2000, and 3000 Hz of the indicated ear (Figure 3). A candidate for Ponto will have an average pure tone bone conduction threshold that is better than or equal to 55 dB HL. Research suggests that if the air-bone gap is greater than 30 dB, then speech recognition is likely to be better with a bone anchored hearing device than with a traditional hearing aid.
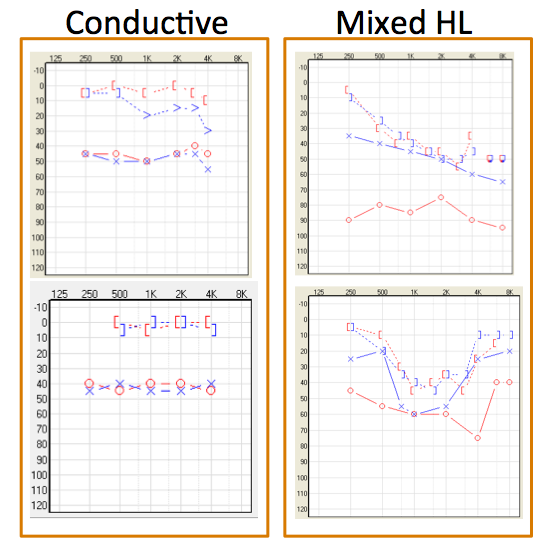
Figure 3. Conductive vs mixed hearing loss.
The audiologic considerations for fitting bilateral bone anchored devices are to have symmetrical bone conduction thresholds (Figure 4). Symmetrical is defined as less than 10 dB difference in average bone conduction thresholds between the two ears, or less than 15 dB at individual frequencies, and in this instance, individual frequencies 500, 1000, 2000, and 4000 hertz.
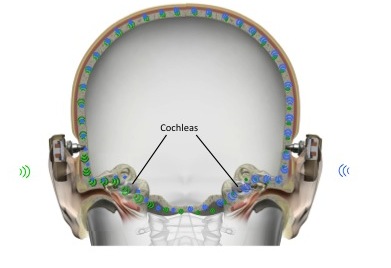
Figure 4. Symmetrical bone conduction thresholds are required for bilateral bone anchored devices.
How does the bone anchored device compare then with traditional hearing aids? Traditional air conduction hearing aids require higher gain, because they have to overcome the air bone gap. With a bone anchored device, you do not need as much gain as traditional hearing aids, because they bypass the middle ear space where the air-bone gap exists. You can achieve better sound quality as a result of the direct bone conduction. In addition, with normal ear anatomy, the ear canal can remain open. If there are problems with draining ears (e.g., chronic otitis media), then a bone anchored device may be the best intervention because the ear canals can remain open.
Unilateral Hearing Loss
What about the child with unilateral profound sensorineural hearing loss on one side with normal hearing on the other? In this application, vibrations are transmitted from the single sided deaf ear to the normal functioning contralateral cochlea. Why consider a bone anchored device in this case? The advantage of the bone anchored sound processor for children with SSD are that it reduces the head shadow effect and increases speech understanding and noise. As Karen Anderson mentions on her website, Supporting Success for Children with Hearing Loss, parents of children with SSD often say, “What is the big deal? The hearing loss is only one ear. The child is doing fine; they are getting good grades.”
Any time listening is a challenge, it is harder for children, especially younger children, with unilateral hearing loss to pick up on new words. In quiet or one-on-one situations, listening to radio or television, and in some loud places (sporting events, theater and shows) children and adults often get by and they appear to be doing fine. For a child with single sided deafness, hearing from a distance and locating sound is also a challenge. This challenge can occur at home, when a parent is talking from another room, or at school when a child is listening to the teacher as they move around the room, and during play activities, as children run around. In these situations, it can be quite difficult to hear and understand when there is hearing loss on one side. Understanding speech in group conversations, identifying speech in noisy settings, and hearing sounds directed to the deaf side are all problematic. Localization helps us to follow conversation. When it takes longer to identify the speaker, the listener may miss some of the message. Localization is also important for safety. If your child is near the street, riding a bike, or even learning to drive, he or she may have trouble localizing a horn.
Research has shown that children with unilateral hearing loss may be 10 times more likely to fail in school. They fall behind and need special help more often, as compared to their average hearing peers. One-third to one-half of children who do not receive help to hear better have problems learning in school. Also, because many rules of social interaction are learned via subtle auditory and visual cues rather than direct teaching, it is not surprising that about one-fifth of these children may ultimately develop behavioral and social issues. Even though a child hears normally in one ear, whenever there is noise or someone speaking at a distance, the child may miss part of what is being said. Learning issues, inside and outside the classroom, are largely due to missing incidental speech that occurs in the environment.
When fitting Ponto on a child with unilateral hearing loss, the audiologic indications are that the child's better ear should be better than or equal to 20 dB HL measured at 500, 1000, 2000 and 3000 Hz. The average air conduction scores need to be good and the child's good ear needs to be within normal limits. Children are considered for bone anchored solutions typically when it has been determined that their bad side, or their affected side, will no longer benefit from amplification provided by traditional hearing aids.
Some children will use a bone anchored device until they outgrow ear infections, or possibly even while awaiting surgery to correct their conductive hearing loss. They may have chronic ear infections, actively draining ears, Eustachian tube dysfunction or very tiny ear canals (e.g., in a child with Down Syndrome). For these children, Ponto on a softband is often used to provide amplification. It might be for a short or long term, but this allows the ear canal to remain completely open, providing better conduction conditions for a dry ear.
Surgical Considerations
It’s important for audiologists to understand the surgery for bone anchored solutions. When parents come in to see the audiologist, they do not only ask questions related to the sound processor. They will also ask you questions related to surgery, such as what happens before and after the procedure. The Ponto surgical procedure is safe and simple. It does not take long and there is no risk of damage to the child's ear or hearing. The surgical techniques have evolved over the years and they continue to evolve. Tissue preservation surgery has become the gold standard in bone anchored hearing implantation. The long-term results show benefit in terms of cosmetics outcomes, reduced numbness around the implant site, and even faster healing.
Wide Ponto Titanium Implant
Our Wide Ponto Implant is designed for maximum implant-to-surface contact with bone for osseointegration to occur (refer back to Figure 2). The shape of our Ponto abutments reduces the body's need to form new tissue in pockets or pathways around the abutment. This means less risk of infection following surgery. Remember, children over the age of 5 and with normal bone thickness are the ones that would be having surgery. Children under the age of 5 are not eligible for surgery; they can wear Ponto on a softband. The shape of our abutments makes it suited for performing the new MIPS procedure, which I will address in just a moment.
Minimally Invasive Ponto Surgery (MIPS)
Like I mentioned, tissue preservation has been further refined. It is the gold standard, and the next step in the evolution is our new Minimally Invasive Ponto Surgery, or MIPS for short. MIPS brings tissue preservation to a whole new level in terms of patient outcomes, which is important for older children. The surgical procedure is a less invasive procedure. It is supported by new tactile surgical components that include a cannula and new state-of-the-art drilling equipment. The MIPS procedure results in minimal disturbance of tissue around the abutment site during surgery. This reduces the body's need to form new tissue around the abutment. By maximizing tissue preservation, the body's blood supply and nerve endings are left as intact as possible.
MIPS not only provides for a shorter healing period, but patients have less post-operative pain and numbness as well. MIPS is a single stage surgery. The FDA approval for MIPS is the same as it is for traditional bone anchored surgery. It includes the same patient groups as for a single stage surgery with our current wide implants and abutments. Those patient groups are: adult patients with normal bone quality and thickness; and, children suitable for single stage surgery with normal bone quality and bone thickness, above 4 millimeters. We take a conservative approach at Oticon Medical so we would say this is generally children approximately 12 years of age and older.
These are some images of MIPS patients one week after surgery (Figure 5). We see nice patient outcomes with no sutures, and no scar.
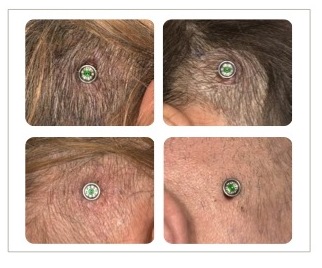
Figure 5. Patient outcomes with MIPS 7 days post op.
The Ponto Biohelix (BHX) Implant is our Wide Ponto Implant that I mentioned earlier, with Biohelix surface modification. The interchannels of every thread of the abutment have been laser ablated. The result is that when the bone grows into the grooves, it creates a faster and stronger bonding to the bone. It is stronger than anything we have ever had in the past. This bonding is about 150 times stronger than if that laser-ablated surface was not present.
Since we first entered the market in 2009, all Ponto abutments have been and still are universal. This aligns with our mission to provide freedom of choice and to put people first. With universal Ponto abutments, if a surgeon implanted a child with a Ponto implant and abutment, the child could use either a Ponto or a Cochlear Baha processor. By doing this, we provide professionals, audiologists, and patients with the freedom of choice when choosing sound processors.
Softband Fittings
Ponto first came on the market in 2009. From the very beginning, we have had advanced technologies and features in the Ponto sound processor. When fitting children, especially children who are not old enough for surgery, they are fitted with Ponto Plus on the softband. Gain and output are important when fitting on a softband, as well as when fitting onto an abutment. Ponto Plus provides the power they need and extended bandwidth to reach the important high frequencies. Being on the Inium platform, Ponto Plus allows for excellent feedback management and connectivity with the Oticon Medical streamer.
Design Features and Fitting Range
Ponto Plus has a design that is durable, reliable, and easy to operate. These features are important when you are working with children, their parents and caregivers, and teachers. The metal spring coupling was designed for durability and ease of use, not only when clicking the processor on and off the abutment, but also for preserving fidelity and sound quality over the life of the instrument. It is a very tight connection but you can easily take it on and off without difficulty.
The battery door is designed to make it easy for parents and teachers to access. It is also tamper resistant. While younger children do not have access to their volume control, the volume control is easy to access for older children. If necessary, volume access can be deactivated in the Genie software. These devices are all nanocoated and carry an IP57 classification for resistance against moisture and dirt. There is also a hole to attach a safety line on the bottom of the Ponto Plus, which is a nice feature. All of our Ponto devices have a two-year repair and two-year loss and damage warranty. An Oticon Medical streamer is standard with Ponto Plus. However, if a family does not feel that they will use the streamer, we can add an additional year repair warranty instead of the streamer. That can be decided upon even 90 days after fitting, if a family comes back for follow-up and finds they are not using the streamer.
Ponto Plus comes in a regular and power model. Figure 6 represents the fitting ranges for both. In terms of average pure tone bone conduction scores, the regular device fits up to 45 dB HL and the Power model fits up to 55 dB HL.
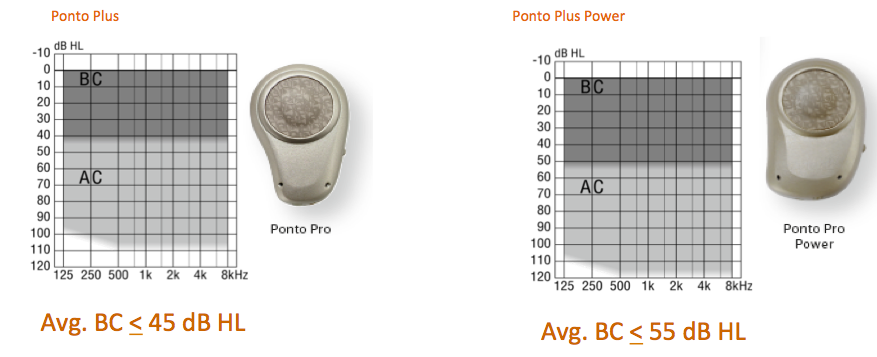
Figure 6. Fitting ranges for Ponto Plus and Ponto Plus Power.
When fitting a child on a softband, you always want to choose the Power model, even if your average pure tone bone conduction scores are 45 dB or better. The reason is because the power device is required to overcome skin and tissue impedance. The same applies for SSD; the Power model should be selected. Even when fitted on an abutment, (not just a softband), children and adults with SSD require a different gain prescription than people with conductive and mixed loss. Even though their bone conduction on the better ear is used, compensation for the transcranial attenuation is added - about 10 to 15 dB more power is needed for the mid and high frequencies.
I just worked with a patient who had SSD. Although the Power model was recommended initially, the regular model was chosen. The patient did not feel it was loud enough and they were much happier when they were moved over to the Power model. Again, we advise the fitting of a power device for your SSD patients, as well as children or adults being fitted on a softband.
Genie Medical Software
For those of you who fit Oticon hearing aids, you will find the Genie software familiar. All Oticon Medical devices are fit with the Genie software, and you can move through the software quickly and efficiently. This allows you more time to spend counseling parents, caregivers and the child.
In the Genie software, when you are selecting the type of fitting, be sure to indicate when you are fitting a child with a softband and/or SSD. It is very important that you tell the software in the fitting screen if you are doing either of these two, or maybe both. The software assumes that Ponto is being fitted on an abutment, and the correction in output and gain is made if you tell the software you are using a softband or fitting someone with SSD. We also recommend measuring BC in-situ, especially if the child is able, and running the feedback manager. A Genie programming quick guide is included in your handout to use as a reference. I have also included a reference sheet for the Oticon Medical regional managers and clinical support staff. We are always happy to assist you and to provide you with training and support.
Factors That Compromise Listening Under Complex Acoustic
Conditions
What are some obstacles throughout the day that make listening and learning more difficult with respect to hearing? The classroom is certainly one place. The acoustic signal degrades with distance and is compromised by background noise. A lot of noise occurs in classrooms. It can also be very noisy at home. Imagine a child sitting at the kitchen counter doing their math homework. The parent is making dinner and quizzing the child for tomorrow's spelling test. At the same time, the dishwasher is running, and the child’s little sister starts to have a meltdown because she cannot watch “Frozen” for the third time today. On top of that, the dog started barking while chasing the cat when the older brother came walking in the door.
We can all envision this scenario and we know how noisy a busy kitchen or a home environment can be. Children with normal hearing can be struggling for full understanding of what is being said in these conditions, so it certainly seems apparent that those with hearing loss are struggling and need access to the best signal possible as well. We think about these situations when fitting traditional hearing aids for children - we should also be mindful of them when we are fitting bone anchored technology.
There are additional factors that compromise a child's ability to listen in complex, noisy environments. Considerable research has been conducted that has found that because children have limited vocabulary and immature language skills, they cannot use context to reconstruct what they have missed via hearing, especially when they are younger. Children’s ability to control attention develops as they get older. Younger children are not as skillful at filtering out unwanted sounds from the sounds to which they should be directing their attention. To be a good listener, especially in noise, children need a rich auditory diet, which younger kids simply do not have. Listening in complex situations is also compromised if a child is in an environment where they are not familiar with the language being spoken (a “non-native” listener). Many of us have worked with children where English is not their primary language.
If you are a child with unilateral hearing loss, it will be much harder to cope in complex listening situations. Greater effort is needed to listen in the classroom, or in an environment where there is a lot going on. Think about the child at the kitchen counter again, practicing for the spelling test. Another example might be a kindergartener – a younger child sitting at a work station, coloring a picture while the teacher is walking around. Another child seated at the same table is making lots of noise. Or, consider the older student in chemistry class, concentrating on the experiment, and following the teacher's instructions. All of a sudden, the careless student in the group drops her beaker on the floor and drama ensues. Listening in these complex situations takes considerable effort and it is a lot of work, and more so for the child with hearing loss.
The goal of providing amplification to a child, even bone anchored amplification, is to improve the signal-to-noise ratio (SNR), provide as much audibility as possible, and give them the best possible representation of sound. The most recent AAA Pediatric Amplification Guidelines (2013) address the use of advanced signal processing in amplification. There have been a lot of changes in technology over the years, and much research to support the use of these advanced technologies as well.
These are just a few statements from the AAA Guidelines as to what is important and why it is important when we fit children with amplification. Fitting amplification to children is much different than fitting adults who may often have acquired their hearing loss later in life after developing speech and language.
- Children are learning language, and do not have the capacity to “fill in the blanks” for sounds that are not audible.
- Children spend most of their time listening to the speech of other children and women, which have greater high frequency content than that of males.
- Children who use hearing aids must develop the ability to use information acquired while hearing amplified, processed sound.
- Children have more demanding listening environments than adults for understanding speech. Enhancement of audibility is required either through increased level, increased SNR, or improvement of the listening environment.
It is important to diagnose hearing loss as early as possible, as the age at fitting of amplification is predictive for speech perception, speech production, and spoken language skills. Furthermore, auditory system development (particularly development of speech perception), is guided by access to relevant acoustic and linguistic information early in life.
Evidence Supporting the Use of Advanced Features for Children
We will now review some research that has helped to support the use of advanced technology for children with hearing loss. These technologies are designed to improve the listening environment. This first study assessed children's performance in complex listening conditions and the effects of hearing loss on the digital noise reduction (Pittman, 2011a). Researchers analyzed a group of children, and their ability to repeat back words in the presence of noise. While the researchers used hearing aids, the big picture results are what are important. Sentence materials were mixed in with background noise before digital noise reduction was applied. After digital noise reduction was applied, the peaks of speech were slightly more pronounced because of the reduction in the surrounding broadband noise at a 0 dB SNR, which is a difficult listening condition.
This study not only looked at speech understanding with digital noise reduction turned on versus turned off, but it was also intended to look at listening effort when listening in noise. In the adult population, there is an increasing body of evidence that shows listening effort can be improved with features like digital noise reduction, even if you do not see an increase in speech intelligibility. Part of the task in this study was to repeat words back while also doing a visual task. The visual task in this study was a connect the dots puzzle that required adding by 3 to get to the next dot (3 plus 3 is 6, plus 3 is 9, plus 3 is 12, etc.). Some effort was needed to be devoted to the visual task, while subjects were simultaneously repeating words presented in background noise.
Performance of children with and without hearing loss was compared across tasks of increasing difficulty: auditory task only; auditory task + visual task; auditory task plus noise; auditory task + visual task plus noise. The last condition included the children with hearing loss only, and that was the auditory task + visual task plus noise, with digital noise reduction on.
For the children with normal hearing, there was some drop in performance from the least difficult to the most difficult task, but not a huge drop. There was a completely different pattern for the children with hearing loss. For each task, they performed a bit more poorly than the children with normal hearing. We know already that for children with hearing loss, it is harder for them in the presence of noise than their normal hearing peers. Statistically, there was no difference in the most difficult task with noise reduction on v. off for the children with hearing loss.
This study does not necessarily show a big difference in word recognition with the noise management on, but it does suggest that noise reduction is one way to reduce background noise to make listening easier.
This next study (Pittman, 2011b) showed more support for the use of digital noise reduction. As stated previously, children use their hearing aids to acquire speech and language, which includes learning new vocabulary. This study looked at the impact of digital noise reduction on a child's ability to learn new words. Children were presented with nonsense words and a picture associated with each nonsense word. The task was to link the new word with the picture. They had no initial training -- they were just given this task of learning new words and were asked to guess what it was.
When comparing the performance with digital noise reduction on versus off, the results are very interesting. After an increasing number of trials, the percentage of words the children could correctly identify was tracked. Children ages 8 to 9 years with normal hearing got better and better the more they were exposed to new words. There was no difference between learning in quiet versus learning in noise. Children ages 11 to 12 years did better than the younger ones. They scored a higher performance level, and again there was not a big difference between learning in quiet versus noise.
For children with hearing loss, that is a much different pattern. The older children with hearing loss never got to the level of that which the normal hearing peers did, and they performed much more poorly in noise than in quiet. The same result was seen with the younger children with hearing loss. A major factor here is the difference between performance in quiet versus noise for the hearing impaired group. Once noise is introduced, it becomes much more difficult for the children with hearing loss to learn new words.
Adding noise reduction for the children with hearing loss made a significant difference.
For older children with hearing loss, noise reduction helps close the gap between performance in quiet and performance in noise. Activation of noise reduction improves the performance in noise for older children, much closer to the level of performance in noise.
For the younger group with hearing loss, interestingly, the activation of noise reduction did not close the gap as much for quiet versus noise like it did with the older children. Dr. Pittman suggests that the SNR improvement in the younger children was not enough to show improvement, but it was enough for the older kids. Turning on the digital noise reduction does not make it worse for children. As children get older, it does make it better. This is certainly support for digital noise reduction – in older children it may have more of an impact, but it never hurts to have it on.
Directionality and Noise Management
In the past, pediatric audiologists had varying opinions about directionality and digital noise management for children (i.e., whether or not it should be turned on or kept off). Dr. Pittman has more research that investigates digital noise management combined with directionality. The updated Pediatric Amplification Guidelines support leaving directionality on, but cautions that you need to have some familiarity as to how the device and the manufacturer implements the feature. Is the device aggressive in implementing noise management, providing comfort but sacrificing audibility? Is it being done in a pediatric friendly way? One of the things that our customers tell us is that they want to feel confident that the device is making the right decision about when to engage these features.
With regard to noise management, Ponto uses a speech-focused noise reduction approach that does a great job of protecting the important speech frequencies. It provides comfort without sacrificing audibility. The effective noise reduction is to allow the child to be in noisy environments without experiencing excessive loudness or fatigue. We want to make sure that children have access to speech cues. First and foremost, identifying the presence of speech in a noisy environment is what the Ponto does, down to 0 dB signal to noise ratio. If speech is present, noise reduction is applied carefully in order to preserve the speech that is there. We do this because the system can determine if speech is there or not -- we do not have to guess. Speech looks very different from noise, so if speech is not present, then noise reduction can be applied a little bit more aggressively.
With regard to directionality, it is essential that the device makes a smart decision as to when to activate, especially for pediatric users. Ponto assesses the signal, tests to see if there could be an improvement in the SNR before automatically activating. If the SNR will be improved, directionality activates. If not, it stays in omnidirectional to preserve sound quality.
Split Directionality, which is in Ponto and in Oticon hearing instruments, provides the benefits of directionality at moderate input levels, not just loud input levels. For most of the time, the benefit of directionality is in improving the SNR above 1kHz, which is exactly what occurs with Split Directionality. With Split Directionality, the low frequencies stay in omnidirectional, and only the frequencies above 1kHz employ directionality, which is the range needed in noisy environments. Full Directionality will engage or employ, but only at louder input levels where we need to provide comfort. Remember, Split Directionality provides improvement at moderate to loud levels. Devices are in Split Directionality more often than Full Directionality. The majority of time, however, children are in omnidirectional mode -- the directionality may not even engage. The system is smart that way. Directionality, whether Split or Full, engages if and only if there will be an improvement to the signal to noise ratio; it will not engage just because it is noisy.
Speech Guard
Unique to Oticon Medical is Speech Guard. Speech Guard is an adaptive compression designed to protect the vital characteristics of the speech waveform. It combines two methods of amplification, slow and fast acting, in a single adaptive compression system. To illustrate, let's take a look at the difference between the adaptive and fast compression in greater detail (Video 1).
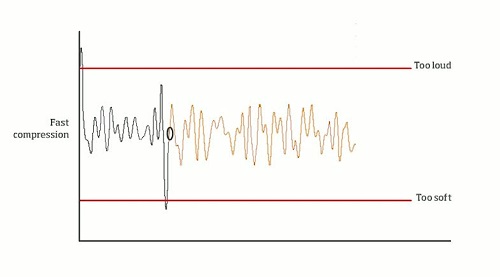
Video 1. Fast compression.
The speech waveform is full of information that the child needs. From the left, what you see is an incoming signal in black and then the output is in orange. Imagine that the compression rate is constantly changing; with fast acting compression it is constantly changing with each alteration of sound. Notice that the fast behavior of the compression system results in a flattening of the output signal, so the intensity variations of the peaks and valleys are diminished.
In comparison, when we look at what is happening in an adaptive compression system such as Speech Guard (Video 2), you will see that there is more of a calm behavior of the compression. It will activate to keep sounds audible and comfortable while the peaks and valleys are preserved in the output signal. Adaptive compression provides both natural sound and comfortable amplification. It also allows for better preservation of speech cues, which is important especially in complex listening environments.
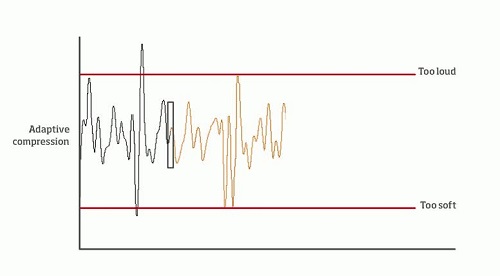
Video 2. Adaptive compression.
Inium Feedback Shield
In terms of feedback management, Ponto Plus is on the Inium platform and uses a very effective, two-stage feedback management system. This is important to preserve the audibility of high frequencies and take advantage of extended bandwidth. Being that the Ponto Plus is on the Inium platform, we have this wonderful Inium feedback management system.
One more study worth noting by Dr. Pittman (2008) looked at the effect of bandwidth on the ability to learn new words. The outcome of this study suggested that children need three times as many trials with limited bandwidth to learn new words, as compared to children who listen via instruments with extended bandwidth. We do not want to manage feedback by reducing access to high frequency sounds and limiting the bandwidth.
Approaches to Bone Conduction
There are two different approaches to bone conduction. The direct drive approach sends vibrations via direct route to bone; the Ponto system is a direct drive system. This is also referred to as a percutaneous approach. With a skin drive approach, vibrations are sent through the skin to bone, which means there is a reduction in the signal due to skin attenuation. This is also referred to as a transcutaneous approach.
When we compare the output of a Ponto Plus device on an abutment to the output of a magnetic skin drive solution, we find that direct bone conduction provides higher output than does a transcutaneous or skin drive solution, both in the low frequencies and in the highs. I’ve talked a lot today about the importance of high frequency information for understanding speech. Increased low frequency information helps to provide better loudness sensation and improved voice quality, so that's important as well.
It is worth noting that when wearing the processors, with both approaches, the processors are worn externally and can be seen. Oftentimes, they are hidden by hair.
Output curves are helpful to compare approaches, but we have also developed a schematic that may be more relatable, especially when talking to parents (Figure 7).
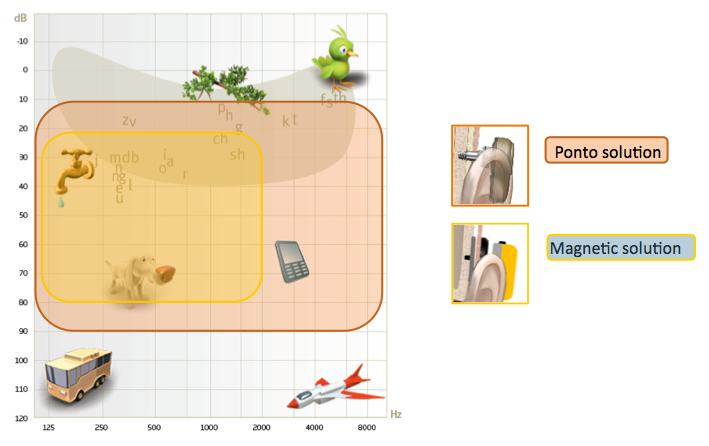
Figure 7. Consequence of skin attenuation on speech phonemes.
When wearing a Ponto on an abutment, what patients can hear is shown in the reddish area in Figure 7. What patients can hear with a magnetic solution is shown by the yellow area in Figure 7. To clarify, this image does not mean that a patient cannot hear sounds above this range; it means that to the patient, the sounds may not be perceived as louder than 70 or 80 dB. As you can see in this schematic, a magnetic solution that attenuates due to the lack of direct vibrator to bone contact will greatly reduce the patient's perception of important speech information. When we look at it this way, it is easy to see the limitations of the magnetic solution in terms of accessing speech cues, especially in the high frequencies.
Summary and Conclusion
Fundamentally, it all comes down to the question of why we are fitting a bone conduction device. Children need to wear a hearing solution that provides maximum audibility in the high frequency region, in order to develop speech and language skills -- inside and outside of the classroom. We believe that a softband is a great choice for children before the age of surgery. After reaching the minimum age for surgery for normal development, the best access to high frequency information is provided through a percutaneous direct approach.
As you think about the children and the families that you serve, what is the goal? Why are they turning to you for help? What are you trying to achieve, and what does the child need? I hope we have a better appreciation for and the knowledge that the Ponto system helps you to help kids achieve the highest degree possible. Please gives us a call or email us if you have any questions. We are always here for you.
Questions and Answers
What is the battery life for the Streamer?
The Oticon Medical Streamer battery should typically last for about 10 hours of use. When used for FM streaming, there is more current drain. For children in the classroom, you can guarantee that you can get a full 8 hours, which is a good day's worth of streaming.
References
American Academy of Audiology. (2013). American Academy of Audiology Clinical Practice Guidelines: Pediatric Amplification. Retrieved from https://audiology-web.s3.amazonaws.com/migrated/PediatricAmplificationGuidelines.pdf_539975b3e7e9f1.74471798.pdf
Pittman, A. (2011a). Children’s performance in complex listening conditions: Effect of hearing loss and digital noise reduction. J Speech Lang Hear Res, 54(4), 1224-39
doi: 10.1044/1092-4388(2010/10-0225).
Pittman, A. (2011b) Age-related benefits of digital noise reduction for short-term word learning in children with hearing loss. J Speech Lang Hear Res, 54(5), 1448-63. doi: 10.1044/1092-4388(2011/10-0341).
Further references in course handout.
Citation
Humitz, M. (2016, May). The Ponto bone anchored system: The right choice for pediatrics. AudiologyOnline, Article 17335. Retrieved from www.audiologyonline.com

