Learning Outcomes
After this course learners will be able to:
- Explain how hearing aid demos contribute to the hearing aid selection and fitting process.
- Describe the main results of the listening test done with hearing care professionals.
Describe the benefits of utilizing an effective hearing aid demo with patients.
Introduction
Hearing Aid Selection: Choosing What’s Best for the Patient
The ideal process of selecting and pre-fitting hearing aids for an adult patient should include individualized assessments of hearing and non-hearing needs, a measure of their motivation and willingness to try hearing aids and setting realistic expectations for hearing aid use (Valente et al., 2007). This approach should include the patient in the decision-making process, with the hearing care professional (HCP) acting as the hearing, technology and fitting expert, and the patient as the expert in their unique needs, lifestyle and budget (Laplante-Lévesque et al., 2010; Poost-Faroosh et al., 2015). In selecting hearing aids for their patients, HCPs are ethically driven, and rely to a great degree on their judgments of a particular brand’s aptitude and image (Johnson et al., 2009). These factors include such elements as product quality and reliability, fit, customer service, innovation and research, product features, and fitting software. HCPs may thus believe that they are acting in a strictly clinical and non-biased fashion in the process of recommending hearing aids. However, this is not the case. In fact, the professional contact between the patient and HCP in and of itself creates a positive bias which can help move patients forward with hearing aids (Naylor et al., 2015). Although bias in science is something to be avoided, it can be an advantage in a clinical situation. One of the professional responsibilities of HCPs is effectively to “sell” their patients on the appropriate treatment course for their hearing loss – most often, hearing aids and professional service. To that end, HCPs use counseling techniques to increase patients’ motivation and likelihood of following the treatment recommendations that HCPs know will improve their hearing-related quality of life. An additional tool that can help is the method that HCPs use to introduce patients to the hearing aids and their confidence in that presentation.
In real-world practice, there will always be a moment of truth when the hearing aids being fit go live on the patient’s ears for the first time. They will immediately be thrust into a foreign sound universe. Regardless of whether they have worn amplification previously, the new hearing aids will most likely sound different than whatever they were used to. At this point, it is critical that the sound quality delivered by the hearing aids creates a positive impression. Wonder, curiosity, surprise, delight – these are the kinds of reactions that transparent sound quality would foster, and that would encourage patients to focus on the valuable guidance provided by the HCP.
Sound quality is personal and subjective and can be difficult to quantify. By using double-blinded methods and trained panels of assessors to help eliminate bias and variability related to idiosyncratic and contextual factors, it has been shown that ReSound LiNX QuattroTM is preferred in terms of sound quality for music and for streaming different kinds of media content (Jespersen et al., 2018; Aranda de Toro & Groth, 2019). Although results from controlled tests like this are useful to substantiate that technical aspects of sound quality can be detected perceptually, no data are as compelling as a personal experience. This applies not only to patients but also HCPs themselves. HCPs can gain valuable insights to what their patients’ initial listening experiences might be like simply by listening to the hearing aids. Knowing what to expect and how the effects might be showcased can help HCPs maximize the motivational potential of those experiences.
Putting Sound Quality to the Test
In a novel experiment designed to put HCPs in the shoes of their patients and to illustrate how sound quality can positively color the initial experience trying hearing aids, ReSound field representatives (“field reps”) were trained to demo ReSound LiNX Quattro hearing aids on HCPs in a similar way that HCPs might do with their patients. To provide further context, HCPs were asked to choose a set of premium hearing aids from another manufacturer and to program them as they would for a patient. These hearing aids were also used in the demo as a basis for comparison. This demo was tested with over 700 HCPs.
Methods
In this experiment, field reps asked HCPs to listen to hearing aids without deliberately trying to influence their experience. Two sets of hearing aids were used. One was ReSound LiNX Quattro and the other was a premium product from another brand chosen by the HCP. The HCP was asked to listen in four listening scenarios using both sets of hearing aids. Subjective ratings of sound quality and objective performance scores were obtained for the listening scenarios.
Sound Sources and Room Setup
The experiment utilized the field rep’s live voice and sound files from a prerecorded library available in ReSound’s Smart Fit fitting software (Sound Player). The sound files were selected based on their relevance to the intended listening environment.
Testing was performed inside a quiet room in the HCP’s office. The room setup included one loudspeaker placed at 0-degree azimuth in relation to the HCP (listener). The loudspeaker was connected to a PC presenting the Sound Player files. The HCP was seated one to three feet from the loudspeaker, depending on room size. The field rep (tester) moved to different positions around the HCP, depending on the listening scenario.
The presentation levels of the test stimuli were chosen to be similar to levels typically found in real-world environments. The field rep verified the loudspeaker level to be approximately 65 dB SPL via a free sound level meter smartphone app (Decibel X). Field reps were directed to use normal conversational levels for live voice presentation.
The listening scenario setups are summarized in the following table and figures.
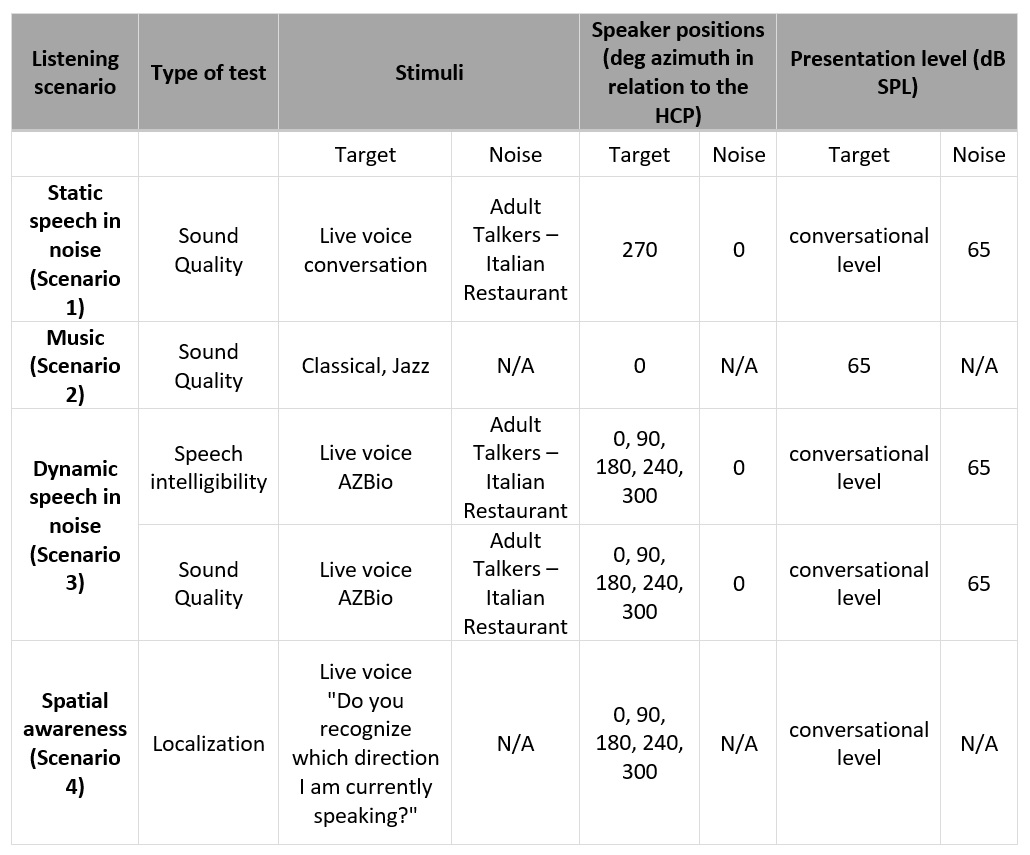
Table 1. Sound and room set up details for each listening scenario.
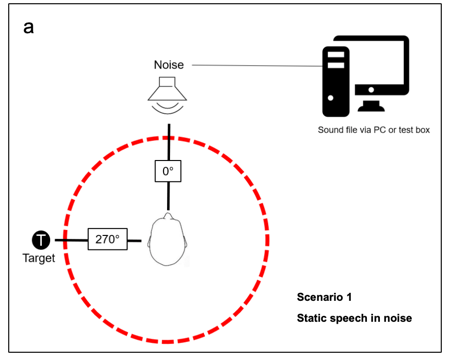
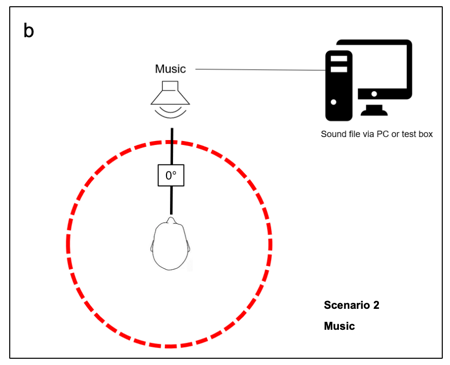
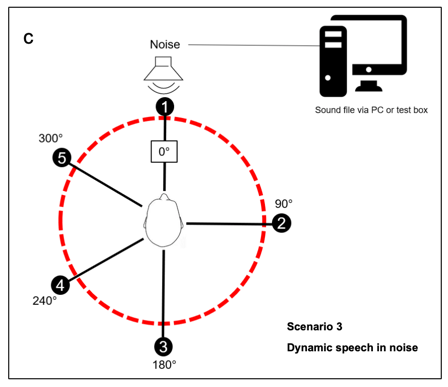
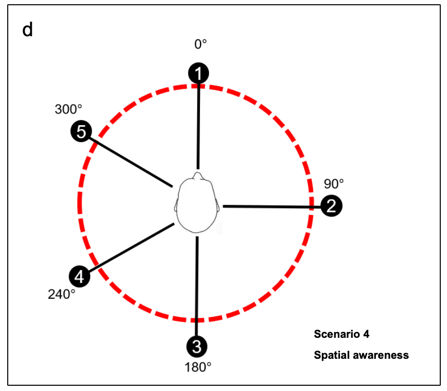
Figures 1a-d. Test setup diagrams for each listening scenario.
Hearing Aid Settings
Receiver-in-the-ear (RIE) hearing aids with medium power receivers were used for all brands. They were programmed with the same bilateral mild-to-moderate symmetrical sloping hearing loss (Table 2). The hearing loss was chosen with the assumption the listener would have normal hearing. These settings, along with use of an appropriately sized power dome, ensured the output of the hearing aids were audible without being uncomfortably loud. A subset of the listeners did have hearing loss, and in these cases, their own audiograms were used.
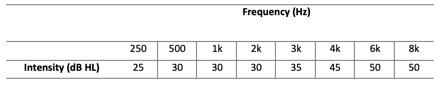
Table 2. Recommended air conduction audiogram for right and left ears for the sound demo.
Before the demo, the HCP created two programs in their set of hearing aids from the other brand. The first program was the default program for general use as recommended by each manufacturer. The second program was for music, again with the manufacturer’s default settings activated. These were the two programs used in the ReSound hearing aids. Examples of features that would be activated in each of the programs are displayed in Table 3.
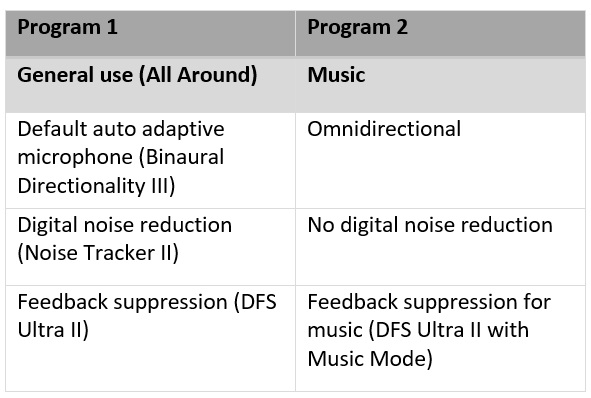
Table 3. Recommended settings for hearing aids from all manufacturers (ReSound settings in parentheses).
Fine tuning adjustments were permitted at the discretion of the HCP, as long as they attempted the same adjustments in both sets of hearing aids. Once the hearing aids were programmed, they were given to the field rep, who then inserted each set of devices onto the HCP’s ears so the HCP would be blinded as to which set of devices they were using.
Listening Scenarios
Static speech in noise (Scenario 1). The HCP was seated facing the loudspeaker as specified in the previous section. The noise source was activated. The general use program was activated in the hearing aids.
The field rep stood to the left side of the HCP and spoke to them. The HCP assessed the sound quality and clarity of their voice. The HCP was asked to rate the sound quality from 1 (poor) to 10 (excellent).
Music (Scenario 2). The hearing aids were switched by the field rep to the music program and the music file was played from the loudspeaker. The HCP was asked to subjectively rate the sound quality of the music from 1 (poor) to 10 (excellent). No noise source was utilized during this scenario.
Dynamic speech in noise (Scenario 3). The HCPs completed a speech intelligibility in noise task, using sentence from the AZBio Sentence Test (Spahr et al., 2012). The hearing aids were set to the general use program by the field rep and the noise source was activated. The HCP closed their eyes. The field rep read one sentence out loud from each of five azimuths around the HCP, and the HCP repeated the sentence to the best of their ability. Five keywords were chosen per sentence, allowing for a total possible score of 25/25. The HCP was also asked to rate sound quality of the field rep’s voice from 1 (poor) to 10 (excellent), which included the HCP’s assessment of ease of listening in noise
Spatial awareness (Scenario 4). The spatial awareness test used the same test setup from scenario 3, with the HCP’s eyes still closed. Instead of asking the HCP to repeat sentences as they move around the listener, the field rep asked “Do you recognize from which direction I am currently speaking?” The HCP pointed in the direction they believed the field rep was standing. For each correct answer, they received one point, for a total possible score of 5/5.
Results
Results for ReSound hearing aids and the other brands’ hearing aids were calculated. The number of observations were not equal for the other five brands, so those results were pooled together in each scenario to create an equal number of comparisons to ReSound devices for statistical analysis. Overall, most responses from HCPs tended to be more positive than negative for all hearing aid brands and scenarios, meaning there was a non-normal distribution of the data (positive skew to the right). The mean scores for sound quality, speech intelligibility and localization abilities favored ReSound LiNX Quattro over all other brands for all listening scenarios. The Wilcoxon signed rank test, a non-parametric test used to compare pairs of data from the same listener, was performed for each listening scenario. The test showed a significant difference between the two hearing aid conditions in all scenarios. These results are summarized in Table 4.
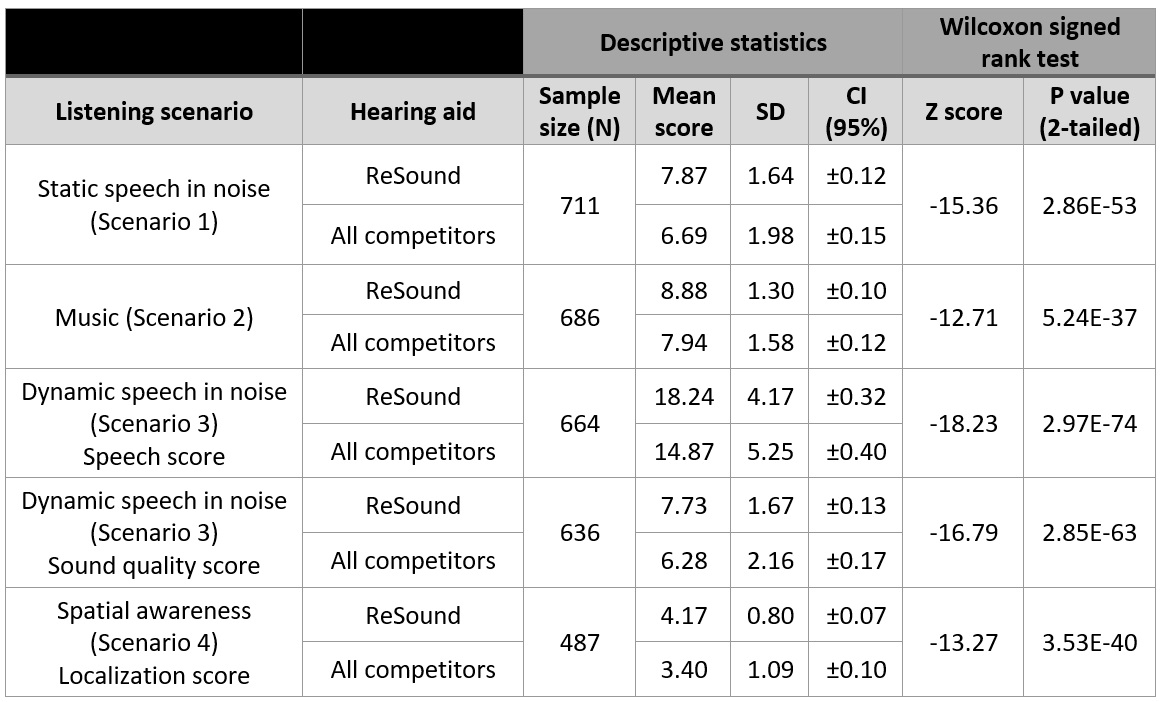
Table 4. Descriptive statistics and Wilcoxon signed rank test results for listening scenario scores obtained with ReSound versus all other manufacturers. Results significantly favored ReSound hearing aids over the other brands in all listening scenarios. SD = standard deviation, CI = confidence interval around the mean.
It is also useful to examine the spread of the data for both hearing aid categories. These results are displayed in Tukey box and whisker plots. Each box displays the middle 50% of all scores in each hearing aid condition (2nd and 3rd interquartile range). Inside each box, median scores are represented by the line, while mean scores are represented by the x. The 1st and 4th quartile ranges are shown via the whiskers. Outlier responses are indicated by points outside the whisker line(s).
Sound Quality
In general, the HCPs gave positive ratings of sound quality for all tested hearing aids across the various scenarios. While some low sound quality ratings were reported, there was greater variability and a wider spread of scores in the 3rd and 4th quartiles, suggesting the majority of responses were more positive.
For both speech scenarios (Figures 2a, 2c), the average ratings for the other brands were less positive than the ReSound ratings. The range and variability of responses for the music condition were much more similar between ReSound and the other brands. Although the ReSound ratings were more positive than those for the other brands, the variability for the other brand category would be expected to be larger, since it included several devices from multiple brands versus the single brand of ReSound.
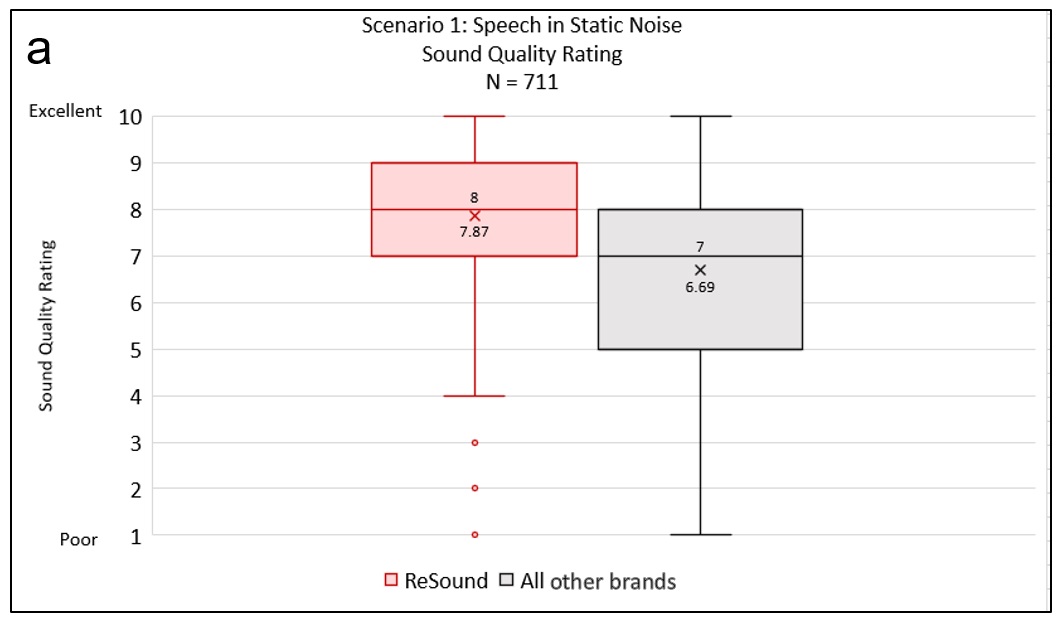
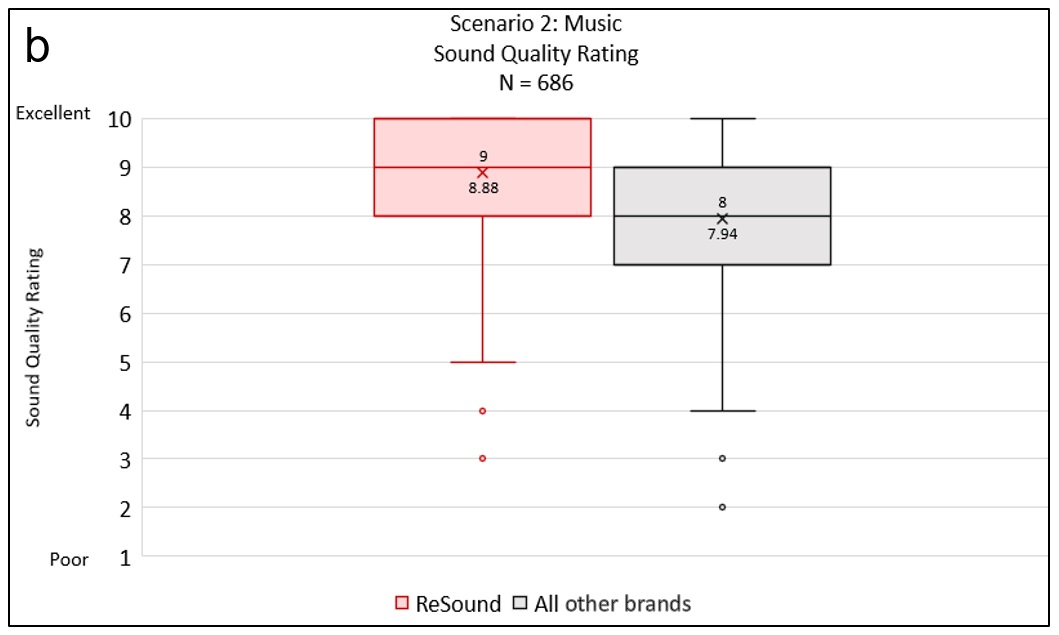
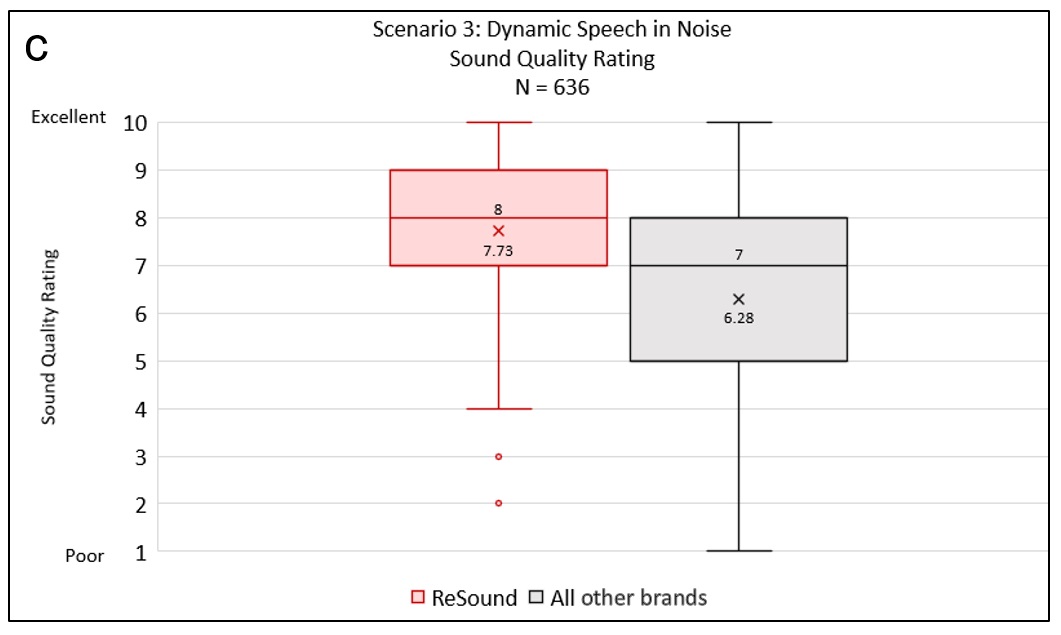
Figures 2a-c. Sound quality scores. Higher scores indicate better ratings for sound quality.
Speech Intelligibility in Noise
Average speech intelligibility scores for the ReSound hearing aid condition were higher and less variable than those scores obtained with the other devices (interquartile range for ReSound = 10-25 versus all other brands = 1-25). This task showed the greatest difference between ReSound hearing aids and those from other brands. While some HCPs did poorly on the task using ReSound hearing aids, those poor performances are outliers, whereas poorer performance with the other brands of hearing aids was more common.
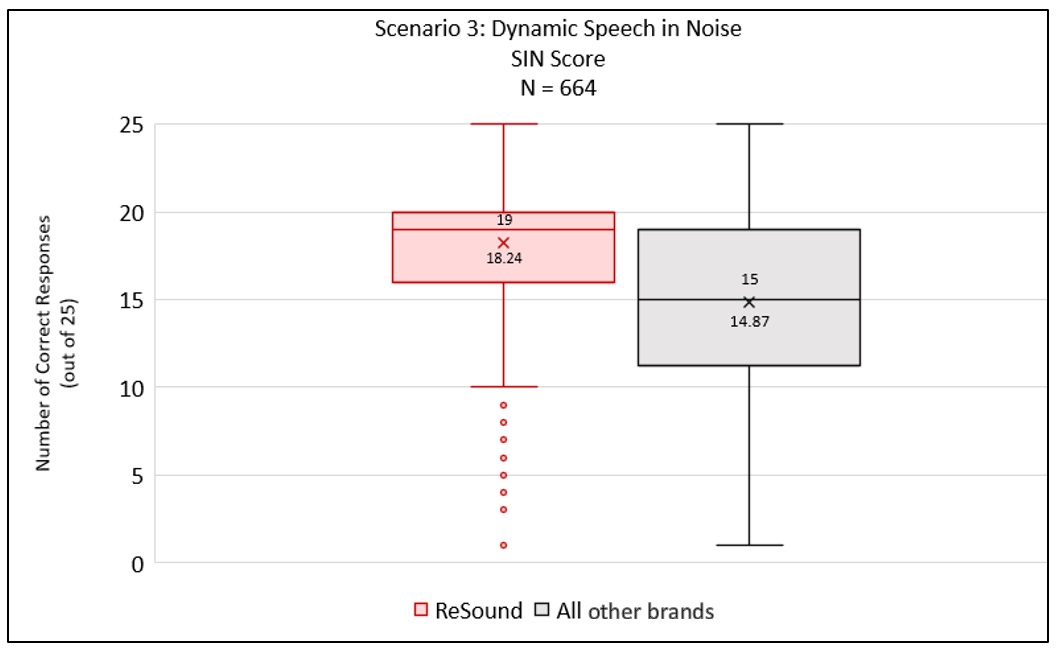

Figure 3. Speech intelligibility in noise scores. Higher scores indicate better speech understanding on the task.
Localization
Overall, responses for the localization task in the ReSound hearing aid condition were higher than for devices from other brands. There was, however, a wide range of variation on the task, suggesting some found it very easy, while others found it to be very difficult.
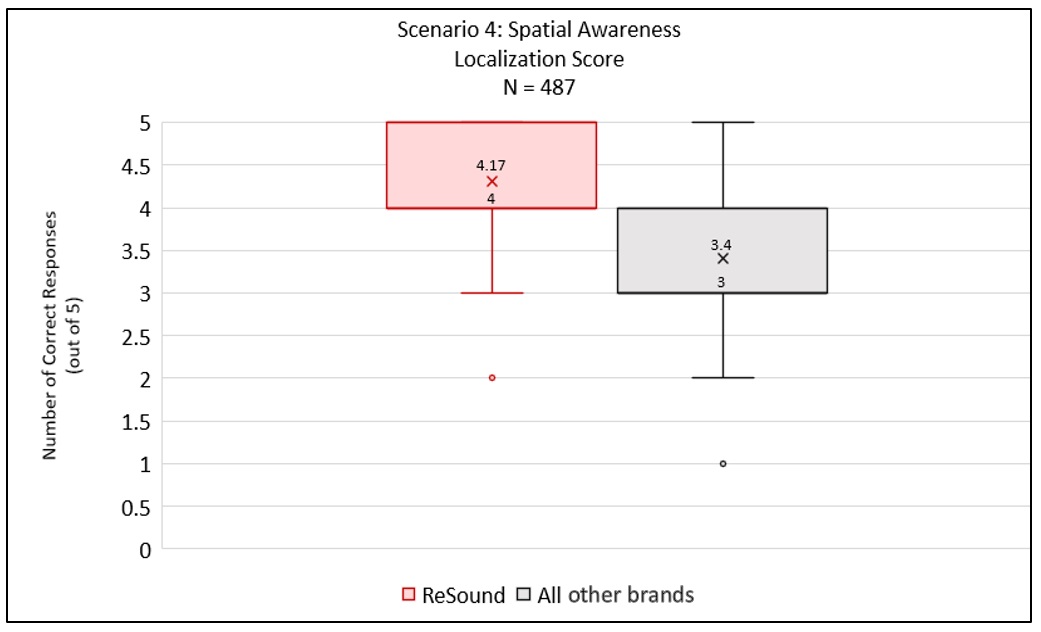

Figure 4. Localization scores. Higher scores indicate better localization abilities on the task.
Discussion
The goal of this listening demo was to provide a practical way for HCPs to listen to and judge different hearing aids, both for their own benefit in gaining an idea on sound quality, intelligibility and localization differences between hearing aids but also so they can pass that knowledge in a more effective way to their patients. Results from testing with over 700 HCPs establishes that it is possible to judge differences in these three attributes across premium hearing aid brands, and that one brand (ReSound) was found to be very positive. HCPs can easily adapt this demo to use with their own patients in order to increase the emotional impact of hearing with hearing aids from the moment they are placed on the patient and to supplement the selection process.
Comments from HCPs
HCPs with normal hearing may have never listened to hearing aids outside of a quiet clinic environment. Several of the HCPs who participated in this demo experienced their first impressions with hearing aids in more complex sound environments. They expressed this was helpful for gaining more insight into the experience of wearing hearing aids. One HCP stated that she was able to better understand what her patients meant when they say what it’s like to “hear but not understand.” Some HCPs commented that they were surprised at how different hearing aids from various manufacturers sounded to them. Comments relating to sound quality of the ReSound LiNX Quattro were expressed using words like “natural,” “clear,” “rich” and “full” when compared to other devices. Differences in own voice quality were also mentioned between hearing aid brands. Note that these keywords relating to sound quality have been shown to be important to users of hearing aids as well (Abrams & Kihm, 2015).
Limitations/Considerations
Average scores from every listening scenario showed a significant advantage for ReSound over hearing aids from other brands. But we must acknowledge that the listening demo described here isn’t a carefully controlled research study. Attempts to reduce bias were built into the protocol, by having the HCP program hearing aids with settings as similar as possible across manufacturers and by blinding the HCPs as to which hearing aids they wore in the listening scenarios. Still, it is uncertain to what extent the field reps could have contributed to bias, even unintentionally. One field rep reported that she had learned to remove the hearing aids from the HCP to change the programs because one of her listeners had pointed out that it was easy to tell what device they were wearing by the audible program change indicators. Other field reps may not have done this, thus giving HCPs an important clue to the test conditions.
However, this is good news for HCPs who want to implement demos like this into their practice. This shows that it is possible to measure sound quality, speech intelligibility and localization abilities using one or more pairs of hearing aids and every day equipment, sound stimuli and a straightforward protocol. The results of a listening experience such as this one can be powerful in showing patients and their loved ones how their hearing could be improved and allows the patient to become more involved in the selection process.
A valid criticism of this demo is the generalizability of the results for actual hearing aid patients because the vast majority of HCPs who participated in the demo had normal hearing. We do, however, have a small subset of data from HCPs with self-reported hearing loss. The HCPs programmed the hearing aids with their own hearing loss. Note there was no further information available on the degree or type of hearing loss. Results for speech intelligibility and sound quality of speech in noise (Scenario 3) suggest that even with hearing loss, the HCPs in this group were able to hear a difference in sound quality between hearing aids, with ReSound devices rated more positively than the competitor devices. A similar result was obtained for the speech intelligibility task, with better scores measured using ReSound devices. The difference in mean scores for both tasks were statistically significant.
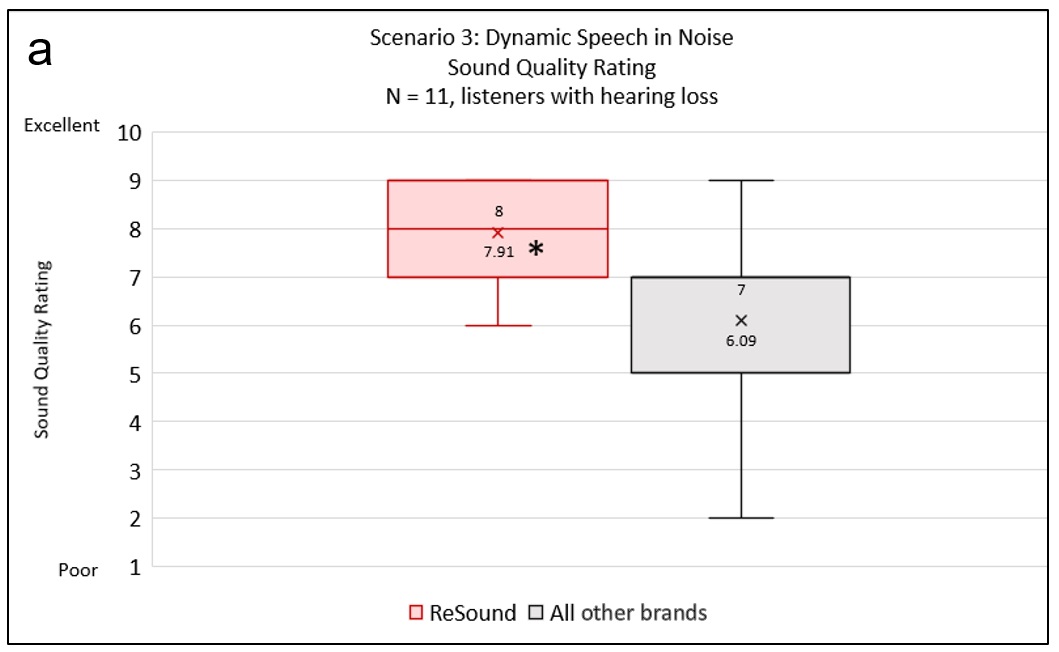
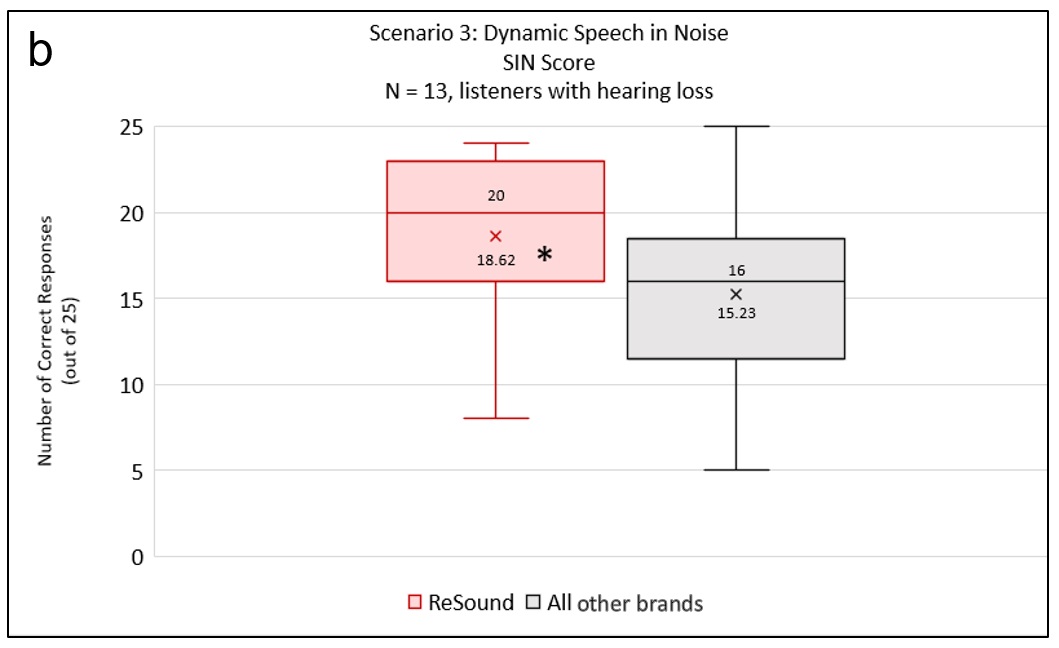
Figures 5a-b. Tukey box and whisker plots for data obtained from HCPs with hearing loss. The asterisk denotes a statistically significant difference in means between the two hearing aid conditions (using the Wilcoxon signed rank test).
These results suggest that HCPs will be able to use this demo with hearing-impaired patients and can reasonably expect them to detect positive aspects of sound quality and to be able to perform listening tasks, at least to some degree.
How Can You Use This Demo?
HCPs should be aware of how they are setting up a listening demo to maximize the wow factor for the patient. It’s also important to keep the demo simple and transparent, so it doesn’t lose its authenticity to the patient and remains as convenient as possible to set up and run. One simple modification that can add a lot of impact for an individual patient is allowing the patient to choose a favorite song for the music portion of the demo. A spouse or loved one who attends the appointment with the patient can be recruited to assist with the live voice portion of the demo, especially the first and last scenarios where only conversational speech is needed.
The protocol length may also be modified, in order to shorten the length of the demo. This occurred in the HCP experiment as well, as can be seen by the varying sample sizes for each scenario. Based on sample size, the static speech in noise sound quality task (Scenario 1) was the most popular, followed by the music task (Scenario 2). Execution of the dynamic environment tasks did take longer and involved a bit more complexity in methodology compared to Scenarios 1 and 2.
Interestingly, this sound demo was originally designed to be used in real-world noisy situations for the dynamic environment tasks (Scenarios 3 and 4). In this case, the tester and listener would go to a café, restaurant or outside next to a busy street and perform the same tasks outlined in the Methods section with the natural sources of noise in place of the sound file. This set up was rarely used (only 6% of the time), so only the results from the indoor setups for Scenarios 3 and 4 were reported. But this setup may be particularly useful for HCPs that have easy access to a noisy place near their office with seating for the patient, such as a cafeteria or shopping center. It may have a stronger impact on the patient, because it is a real-life scenario. If a patient reports a specific environment is causing difficulties in noise during an assessment of hearing handicap, this may also shed light on appropriate environments for a demo or comparison outside of the office.
The listening demo may need some tweaking to be most impactful for patients who have hearing loss. As shown above, the demo can result in similar experiences for hearing impaired listeners as those with normal hearing, but there can be a wider variation in listener responses based on the severity of their hearing loss and other factors. Patients with more severe hearing loss may not be able to perform the speech intelligibility in noise task, for example. However, it is still possible to give any listener the chance to assess sound quality in a variety of listening situations, and to let patients who haven’t yet tried hearing aids a chance to see what amplification can do for them.
What Does This Mean for Your Fitting Practices?
Imagine the impact a sound demonstration could have on a patient who is still not sure hearing aids are right for them. Instead of relying on the HCP’s description of hearing aid features, or the different levels of technology, the patient instead walks away with a real demo of what these sounded like. It is a powerful tool in the HCP’s tool box to be able to demonstrate both better hearing and sound quality, not just talk about what that may sound like once the patient invests in hearing aids. The experiment described in this paper suggests that it is feasible to routinely conduct this sound demonstration and that it does in fact demonstrate sound quality attributes typically described with hearing aid use. Evidence supports hearing aid users’ expectations for hearing aids are predictive of satisfaction (Meyer et al, 2014). Saunders et al (2009) used an experimental design to compare outcomes when fitting did or did not include pre-fitting counseling. The pre-fitting counseling was done either with or without a live demo. They found a positive effect of both methods of pre-fitting counseling compared to no counseling, which supports the common clinical approach of aligning patient expectations with what is realistic. They further reported that, although it wasn’t a quantified outcome of their study, participants spontaneously indicated that they enjoyed the live demo and listening experience. This suggests that patients can integrate both the information relayed to them from the HCP along with the emotional experience of using hearing aids in a demo in order to help them make their decision about hearing aids.
Acknowledgment
We would like to thank Dorea Ruggles, GN Advanced Science, for her assistance with the statistical analysis in this paper, and Hans Christian Dreschler, GN Education & Training, for creating the demo used in the study.
References
Abrams, H.B., & Kihm, J. (2015). An Introduction to MarkeTrak IX: A new baseline for the hearing aid market. Hearing Review, 22(6), 16-21.
Aranda de Toro, M., & Groth, J. (2019). Independent study shows that ReSound LiNX Quattro is preferred for direct audio streaming. ReSound white paper.
Jespersen, C.T., Kirkwood, B., & Groth, J. (2018). Evidence for clearer, fuller and richer sound quality with ReSound LiNX Quattro. ReSound white paper.
Johnson, E. E., Mueller, H. G., & Ricketts, T. A. (2009). Statistically derived factors of varied importance to audiologists when making a hearing aid brand preference decision. Journal of the American Academy of Audiology, 20(1), 40–48.
Laplante-Lévesque, A., Hickson, L., & Worrall, L. (2010). Factors influencing rehabilitation decisions of adults with acquired hearing impairment. International Journal of Audiology, 49(7), 497–507.
Meyer, C., Hickson, L., Khan, A., & Walker, D. (2014). What is important for hearing aid satisfaction? Application of the expectancy-disconfirmation model. Journal of the American Academy of Audiology, 25(7), 644-655.
Naylor, G., Öberg, M., Wänström, G., & Lunner, T. (2015). Exploring the effects of the narrative embodied in the hearing aid fitting process on treatment outcomes. Ear and Hearing, 36(5), 517-26.
Poost-Foroosh, L., Jennings, M. B., & Cheesman, M. F. (2015). Comparisons of client and clinician views of the importance of factors in client-clinician interaction in hearing aid purchase decisions. Journal of the American Academy of Audiology, 26(3), 247–259.
Saunders, G. H., Lewis, M. S., & Forsline, A. (2009). Expectations, prefitting counseling, and hearing aid outcome. Journal of the American Academy of Audiology, 20(5), 320-334.
SkyPaw Co. Ltd (2019). Decibel X: dB, dBA Noise Meter (Version 7.0.0) [Mobile application software]. Retrieved from https://apps.apple.com/us/app/decibel-x-db-dba-noise-meter/id448155923
Spahr, A. J., Dorman, M. F., Litvak, L. M., Van Wie, S., Gifford, R. H., Loizou, P. C., … Cook, S. (2012). Development and validation of the AzBio sentence lists. Ear and Hearing, 33(1), 112–117.
Valente, M., Abrams, H., Benson, D., Chisolm, T., Citron, D., Hampton, D., … Sweetow, R. (2007). Guidelines for the audiologic management of adult hearing impairment: American Academy of Audiology Task Force. Retrieved from https://audiology-web.s3.amazonaws.com/migrated/haguidelines.pdf_53994876e92e42.70908344.pdf
Citation
Schumacher, J., Buemi, M. & Groth, J. (2019). The Power of the Demo: An Innovative Field Study Offers a New Perspective. AudiologyOnline, Article 25684. Retrieved from https://www.audiologyonline.com



