Question
There are times during speech-mapping hearing aid verification, when I need a bit more gain to match target, I increase gain in the hearing aid fitting software in the higher frequencies, but I don't see any increase in the real ear aided response output. What's going on?
Answer
It’s certainly tempting to think that there is something wrong with the software, the hearing aid, or maybe a procedural problem with the probe microphone. The most probable reason for this finding, however, is that the fitting is open and you are using the incorrect equalization method. This is sort of old news, as Todd Ricketts and I published a paper on this 12 years ago, but maybe the message never found its way to you.
Historically, going back to the 1980s, we've typically used concurrent equalization. Concurrent equalization means that the reference microphone is continually on, and is continually monitoring the output signal. This loop enables it to maintain the output signal at whatever level you set it, and its constant monitoring allows for corrections of minor head movements. This is the default equalization procedure in most, if not all, probe-mic equipment.
There is a second equalization option called stored equalization. With stored equalization, you calibrate everything initially, but then you turn the reference microphone off. While you're conducting your testing, it is not calibrating. With stored equalization, the patient can't move his head because you have calibrated it to one specific place. With most probe equipment, since concurrent equalization is the default, you have to actively select something in the probe-mic fitting software to change to stored equalization. Stored equalization is used with open fittings, so depending on what equipment you use, you may have to select "open fitting" or "open" or something similar in the software in order to use stored equalization—check with your manufacturer if you’re not sure how to access this setting.
So back to your question—What happens if you forget to do this and you accidentally use concurrent equalization with a patient who has a relatively open fitting? Amplified sound will leak out of the ear canal and be picked up by the reference microphone which is still active. If you have the hearing aids set to 15 dB of gain or more, which is usually the case, it is very possible that this sound leaking out of the ear is greater than the sound coming out of the loudspeaker. The reference microphone thinks the sound leaking out of the ear is output from the loudspeaker, and automatically reduces the input. You think you are using the input you selected on the screen, when actually the reference mic is actively reducing the input because it's responding to the sound leaking out of the ear. On your screen, the result will be less than the true hearing aid output. The more you turn up the gain, the more sound leaks out of the ear. The more sound that leaks out, the more the reference mic turns down the input.
Several factors will affect the magnitude of this error. The more gain you have in the hearing aid, the greater the likelihood this will happen, and the bigger the mistake. The better your feedback reduction system is in the hearing aid, the more likely this will happen because it will allow you to put in more gain. How open your fitting is will also affect this, because you will see this effect at the residual ear canal resonance of the patient. So, if you have a very open fitting, you'll likely maintain nearly all of the patient's ear canal resonance, which is typically in the area of 2000 - 3000 Hz, and that's where you will usually see this mistake (i.e., if the ear canal resonance is 20 dB, this will be added to the amplified input signal for this frequency region).
In Figure 1, I show a case where I used both the correct equalization (stored; pink curve) and the incorrect equalization (concurrent; green curve) for an open fitting. As you can see in Figure 1a, with the concurrent equalization, the result was an almost perfect fit to target, except for a 5 dB dip at 3 kHz. Being a prudent target-fitting audiologist, I'm going to start turning up gain to see if I can hit the 3K target. With the equipment still set to concurrent equalization, I raised gain until I nailed my target at 3 kHz. Then, I went in and used the correct equalization - stored equalization - to see the actual output in the ear, shown in Figure 1b. You see by the pink curve in Figure 1b, that using the incorrect equalization would have resulted in a very serious mistake in this case - overshooting the target by about 18 dB. I have heard people say that the NAL-NL2 is too tinny and causes feedback. Well, in many cases, the problem may be that the wrong equalization procedure was used, resulting in 15 to 20 dB more gain or output than what the fitter thought they were getting, and the fitting was nowhere near the NAL-NL2 targets.
It is critical to pick the correct equalization, and with open fittings the correct choice is stored equalization. You also can use stored equalization with closed fittings if you want to - just remember that once you have the equalization stored, then the patient can't move his or her head during your measurements.
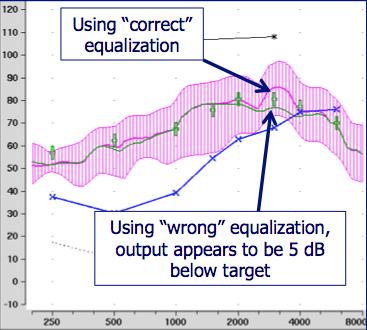
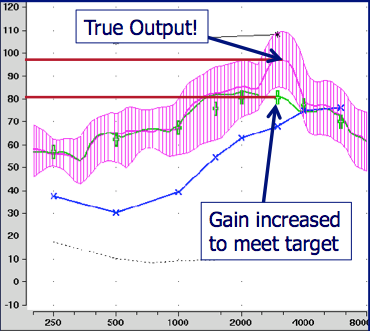
Figure 1a (left) and 1b (right). Using stored equalization (pink curve) and concurrent equalization (green curve) with an open fitting. Using concurrent equalization with an open fitting can result in the erroneous conclusion that the output is below target (Figure 1a, green curve). This error is further confounded if the fitter compensates by increasing gain and overshooting the target (Figure 1b).
Okay, that all makes sense, but here is a follow-up question. What if I'm using the correct equalization, and I see something similar - then what?
So what if you are seeing this same problem, but you know it has nothing to do with the type of equalization? Again, there could be a couple different reasons for this, but my first thought would be to consider your MPO settings. In particular, if increasing gain does not result in a change, or only a minimal change in the REAR only at the highest input level, which is usually around 75 dB, your observation could be related to the MPO. This means you might want to take a look at the REAR85—as measure that once was called the RESR (real ear saturation response), but in the most recent ANSI standard it's been changed to the REAR85 (or REAR90 if you use that input level). That is the brown line in Figure 2 and is a swept tone, usually conducted at 85 dB SPL.
The white asterisks at the top of the graph connected by the white line are the measured, frequency-specific loudness discomfort levels (LDLs) at 500 Hz, 1500 Hz and 3 kHz. It is important to measure frequency specific LDLs to determine the targets, as the REAR85 should fall 5 dB or so below those levels. Do not use average LDLs as there is a very wide range of "average" and you may well be off the mark for your individual patient. The MPO fitting in Figure 2 is a pretty good match to target (just below measured LDLs). You have multichannel AGC-O, so at 1k Hz, I would take the kneepoint and lower it about 5 dB so that the 85 dB SPL swept tone curve falls below the LDLs about 5 dB all the across the spectrum.
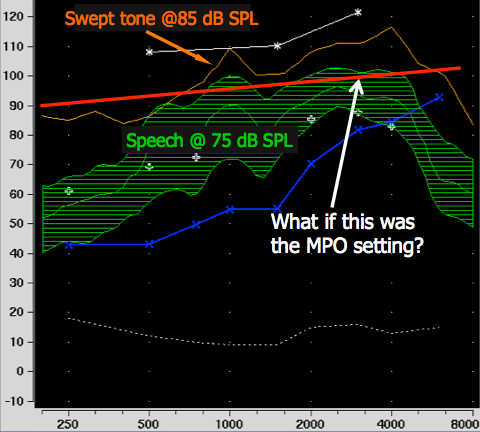
Figure 2. Consider the relationship between the MPO setting and the peaks of speech.
The teaching point here relates to the earlier problem: If you have very low MPO settings, as you raise the gain of the instrument, you may not see an increase in the REAR, simply because you're bumping up against the AGC-O. In this case, you would have to decide whether the MPO is set correctly, and then decide how to manage the issue. What you'd normally want to see is a very systematic separation between your REAR curves for soft, average and loud inputs. If you have roughly the same distance between the soft and average curves as between the average and loud curves, you're likely in good shape.
