
Introduction
Today's hearing instruments are available at various levels of sophistication. As a hearing care professional, you are faced daily with the challenge of selecting those hearing aids that are the best match for the individual patient’s needs in terms of affordability, technologic sophistication, special features, quality, benefit, and satisfaction. Hearing aids can be a major expenditure, so the potential benefits of advanced instruments have to be weighed against the higher costs in each individual case.
Most hearing care professionals would agree that the primary motivation for acquiring hearing aids is to obtain improved speech intelligibility for the vast majority of the users. So one question you might reasonably ask yourself when balancing cost against potential benefits is whether the sound quality of the hearing aid is important enough to be part of the equation, or whether it is best regarded as a nonessential “nice-to-have.”
A recent MarkeTrak survey (Kochkin, 2010) indicates that sound quality is, in fact, a primary factor in relation to hearing aid satisfaction. Of the 10 most important factors found to influence overall user satisfaction, 5 were related to sound quality (clarity of sound, natural sound, richness/fidelity of sound, comfort with loud sounds, sound of own voice (occlusion). Moreover, the MarkeTrak V study (Kochkin, 2000), which comprised a large-scale investigation of the reasons why some hearing aids end up in the drawer, indicated that the sound quality of the hearing aid can be decisive for whether a hearing aid is accepted or rejected by a patient. In this study, poor sound quality was the eighth most common reason given by hearing aid candidates for not using their hearing aids. Thus, with potential benefits of higher user satisfaction, fewer returns, sometimes less need for fine-tuning and consequently fewer visits to the clinic, selecting hearing aids with a high sound quality seems a logical thing to do. The next question is, “What characterizes a good hearing aid sound quality?” This will be discussed in the following sections.
Design Requirements for a Natural Sound Reproduction in a Hearing aid
Hearing aid manufacturers are able to shape the sound quality of their devices by adjusting a number of parameters. When talking about Widex hearing aids in general, we often refer to “The Widex Sound” as a special signature or trademark of Widex. The Widex Sound is the sum of a number of choices made during the development process and the signal processing chain in the hearing aid to obtain the sound quality we believe to be optimal for the wearer. The following sections elaborate on the key variables we know to be important for a good hearing aid sound quality and discuss the design parameters we have chosen to implement in order to provide the best possible sound quality for the wearers.
Short Delay between the Hearing Aid and Natural Sound
Keeping the delay between direct and processed sound short is an important design requirement when aiming for a good sound quality. Hearing aid users with good hearing in some part of the frequency range will often hear both the sound which has been amplified through the hearing aid and the sound that enters the ear canal directly through the earmold or eartip. Perceptible artifacts will begin to occur when there is a delay greater than 10 ms between direct and processed sound. Similarly, a delay between visual and audible input which exceeds 150 ms means that the synchronization between them will be lost (e.g. lip synchronization between TV image and TV sound). The perceptual consequences of different delay times are illustrated in Figure 1.
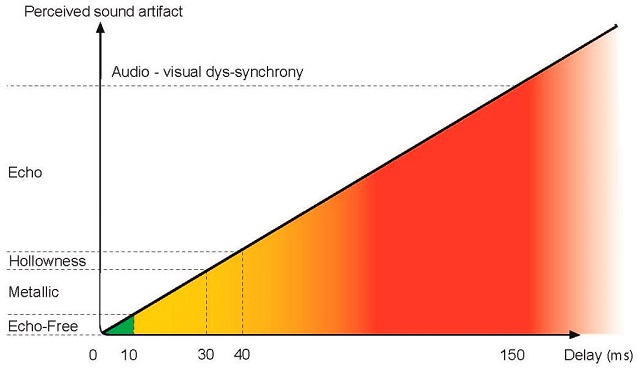
Figure 1. Perceptual consequences of different delay times. Delays as short as 10-30 ms between direct and processed sound will result in a metallic sound quality. Similarly, delays longer than 150 ms may result in a dys-synchrony between the visual and audio signals.
A recent study of speech intelligibility when listening simultaneously to a direct signal and a delayed signal through a wireless system showed that a delay of more than 20 ms could damage the speech intelligibility (Whitmer, Brennan-Jones, & Akeroyd, 2011). Even delays longer than 5-10 ms in a hearing aid may have a negative influence on the sound reproduction in a hearing aid (Stone & Moore, 1999).
A delay between high and low frequencies can also be important. If the high frequencies arrive in the hearing aid user’s ear before the low frequencies, artifacts in the form of short, high-pitched chirp sounds may be heard as a result. Research has shown that a delay greater than 9 ms across the frequency range will be perceived as disturbing (Stone & Moore, 2003).
Consequently we aim to keep the total delay through the hearing aid as low as possible, and at least below 10 ms. This is illustrated in Figure 2, which shows the delay across the high, low, and mid frequencies in a Widex DREAM RIC device.
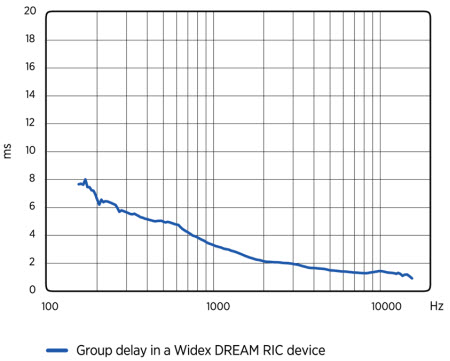
Figure 2. The delay across the high-, low-, and mid-frequencies in a Widex DREAM RIC device. The general aim is to keep it as low as possible, and at least below 10 ms.
High Dynamic Range for a Faithful Reproduction of all Sound Levels
For many years, the focus of the hearing aid industry has been on improving speech perception in different environments, while other inputs, such as music, have been a secondary consideration. Therefore, most hearing aid manufacturers historically have chosen a design where the upper limit of the hearing aid’s dynamic range was located just below 100 dB SPL, in view of the fact that even if you shout, the loudest speech components will usually be within 85 - 90 dB SPL (Chasin, 2007). However, even though all levels of speech may be covered by such a dynamic range, more intense inputs, such as live music or speech produced in the presence of loud noise, may be distorted because they exceed the upper limit.
Chasin (2007) measured a wide variety of musical instruments and reported the range of average sound pressures to be between 60 dBA and 110 dBA, with a few instruments reaching 118 dBA. The peak levels of these instruments were between 94 dB SPL and 118 dB SPL, with a few going as far up as 126 dB SPL. Symphonic music was found to have average levels of 86 to 102 dBA, with peaks between 120 and 137 dB SPL, while amplified rock music was even more intense with averages of 102 to 108 dBA and peak levels above 140 dB SPL.
The human ear will start distorting sound at very loud levels. Sound levels in excess of 110 dB SPL will normally be perceived as somewhat distorted by a person with normal hearing (Killion, 2009). This suggests that in order to offer a natural sound reproduction, the upper limit of the hearing aid’s dynamic range should reach at least up to 110 to 115 dB SPL. This is also supported by Chasin (2003) who measured input limiting levels in relation to optimal reproduction of music. He found that the level should be at least 105 to 115 dB SPL. Our most recent hearing aid series, the Widex DREAM, has therefore been designed in such a way as to provide a dynamic range with an upper limit of approximately 113 dB SPL.
Wide Frequency Range for a Faithful Reproduction of Both Low- and High-frequency Sounds
The frequency bandwidth, or the widest range of frequencies that can be reproduced faithfully through the hearing aid, has an impact on the perceived sound quality.
For the vast majority of hearing aid users, the primary motivation for wearing hearing aids is to achieve improved speech perception. Historically, a frequency bandwidth of 5 kHz was considered more than sufficient, since early studies on telephone conversations indicated that an upper limit of approximately 3 kHz was sufficient for normal-hearing listeners to be able to understand speech (Boothroyd & Medwetsky, 1992). However, as pointed out by Boothroyd and Medwetsky (1992), there is an inherent danger in extrapolating results from normal-hearing listeners to listeners with sensorineural hearing loss, who are highly sensitive to less-than-ideal listening conditions with (e.g. low signal levels and noisy, reverberant surroundings), and whose ability to take advantage of linguistic and semantic redundancies of running speech is reduced as a result of their sensorineural damage. Even normal-hearing listeners have trouble perceiving low-redundancy stimuli with a bandwidth of 3 kHz.
Moreover, later studies on the frequency content of speech have shown that a relatively large proportion of useful speech cues are found above 3 kHz. For the majority of English fricatives, the voiced and voiceless cognates of ‘s’, ‘f’, ‘th’, and ‘sh’ (/s, z, f, v, θ, ð, ∫, Ʒ/), the most important cues are located above 3 kHz. The phoneme /s/ and its voiced cognate /z/, are among the most commonly occurring consonants in the English language, and are used are used for a number of grammatical purposes, including the marking of plurals, possessives, the third-person singular tense and contractions (Yavas, 2006). Jongman et al. (2000) found the mean spectral peak location of /s/ and /z/ to be located around 7.5 kHz when produced by female speakers, and around 6.2 kHz when produced by male speakers. Moreover, a recent study by Todd et al. (2011) found an average spectral mean of approximately 7.7 kHz in children aged 2 to 9 years, with spectral peaks reaching 10 kHz in some of the children. Such findings have resulted in a change of attitude towards the importance of bandwidth; the recommendation nowadays is that an upper frequency limit of 8 to 10 kHz is desirable in order to provide audibility of speech sounds with important high-frequency cues (Stelmachowicz, Pittman, Hoover, & Lewis, 2001; Stelmachowicz, Lewis, Choi, & Hoover, 2007).
Recent research suggests that hearing aid bandwidth is important, not only for speech perception, but also for subjectively perceived sound quality. For example, a study comparing a frequency range of 5 kHz with a frequency range of 16 kHz when listening to music revealed that the majority of the 12 hearing-impaired judges were able to hear the difference and preferred the wider bandwidth (Killion, 2009). Similar results were obtained by Moore and Tan (2003) with normal-hearing listeners. Their study revealed a progressive decrease in perceived naturalness of music as the upper frequency limit decreased from approximately 16.8 kHz to 3.5 kHz. Interestingly, there was also a marked degradation for the naturalness of speech as the upper frequency limit decreased from approximately 10.8 kHz. The typical telephone bandwidth of 313 to 3547 Hz resulted in very poor quality. Moore and Tan (2003) also found evidence to suggest that the lower the cutoff frequency in the lower frequencies, the higher the perceived naturalness of music and speech.
It should be noted that the wide bandwidth ranging from approximately 100 Hz up to 10 kHz in state-of-the-art, high-end hearing aids like the Widex DREAM, will mainly be useful to hearing aid users with reasonably good residual hearing at the upper and lower ends of the frequency range. For example, hearing aid users with severe-profound hearing loss and/or dead regions in the higher frequencies are unlikely to benefit from an extended bandwidth in the high frequencies as their hearing is typically too damaged in those frequencies to derive benefit from hearing aid amplification. For those hearing aid users, frequency shifting may be a good alternative.
No Unintentional Introduction of Artifacts
In order to achieve a high sound quality, the hearing aid must reproduce sound signals with a minimum of distortion and noise. Distortion is defined as alteration of the original signal that will make sounds harsh or sharp and reduce the intelligibility of speech signals. Noise, on the other hand, does not originate from the original signal. It is an unwanted introduction of sound that may result in the masking of other wanted sounds. Noise can be introduced intentionally, as in the case of tinnitus treatment, but generally is an unwanted byproduct introduced by the signal processing or the hearing aid components if not carefully designed.
As mentioned above in the section on the importance of a high dynamic range, distortion in the form of peak clipping may occur if the upper limit of the hearing aid’s dynamic range is too low for intense inputs like live music.
The speed with which gain regulations are made by the compression system in response to changes in signal level may also result in distortion if not carefully implemented. A hearing aid compression system may have fast or slow regulation (or attack and release times) depending on the manufacturer’s choice. One advantage of fast regulation is that it enables the compressor to respond to very brief changes in the environment. In situations where speech and background noise compete, gain is regulated with sufficient speed to raise the soft portions of the speech signal above the hearing threshold when they fall in the dips of the background noise. This may have a beneficial effect on the wearer’s speech perception. However, fast regulation will also cause background noise to be amplified during brief pauses in the speech signal, resulting in a “pumping effect,” which may be perceived as annoying by the listener. Thus, fast regulation may result in both increased speech intelligibility and annoyance.
Of course, one could argue that the regulation speed which provides the highest speech intelligibility should always be implemented, since the primary motivation for wearing hearing aids is to improve speech intelligibility in most cases. However, fast regulation may also have a detrimental effect on speech perception, known as spectral and temporal smearing. When this effect occurs, the natural spectral (i.e., frequency/intensity) and temporal (i.e., time/amplitude) contrasts between speech components are reduced. Examples of consonant confusions occurring as a result of fast regulation have, for instance, been found in several studies (e.g., Hedrick & Rice, 2000; Jenstad & Souza, 2005).
A hearing aid with slow regulation cannot respond quickly to changes in intensity. However, with longer regulation times, the natural contrasts between different speech components are better preserved. Studies on subjectively perceived sound quality have shown that hearing-impaired listeners tend to prefer the sound quality generated by slow regulation to the sound quality generated by fast regulation (e.g., Gatehouse, Naylor, & Elberling, 2006; Hansen, 2002). Thus, even though fast regulation may improve speech perception in some situations, hearing aid users are probably best served with slow regulation most of the time. One possible solution is to implement a predominantly slow compression system that temporarily permits faster regulation in specific situations, such as abruptly changing sound environments, where slow gain regulation may not provide sufficient audibility of soft sounds and protection from sudden loud sounds. Such a system is available in all hearing aids by Widex.
Widex puts forth a substantial effort to ensure acoustic transparency - hearing aid sound which is as close as possible to the original sound source without audible artifacts. All hearing aids are tested thoroughly for unwanted artifacts before being released for sale. Some distortion products and delays can be measured, while others cannot be detected via objective measurements. To ensure that the latter are discovered, the sound quality of Widex hearing aids is tested both by means of objective measurements and an internal panel of trained listeners, consisting of both normal-hearing and hearing-impaired listeners with many years of experience assessing hearing aid sound quality and listening for artifacts.
On a final note, it should be pointed out that while most changes of the original signal that may occur in a hearing aid are unintentional and unwanted, there are exceptions where the benefits of the altered signal are judged to outweigh the drawbacks. The most obvious example is the digital signal processing which performs intentional distortion of the original signal by amplifying signals at certain frequencies to compensate for the hearing loss. Another example is frequency shifting. This technique is used to provide audibility of high-frequency information for people with severe-to-profound or precipitously sloping high-frequency hearing loss whose cochlear high-frequency region is so severely damaged that it is not possible to restore audibility by means of conventional amplification. Audibility is achieved by shifting the high-frequency information to a lower frequency region with some residual hearing. Manufacturers employ different techniques to achieve this end; regardless of the technique used, the sound produced by the frequency lowering algorithms will inevitably sound unnatural at first and require acclimatization and training.
The Fitting Rationale – Another Contributor
In addition to the technical design parameters, another important contributor to sound quality is the fitting rationale, or the algorithm that automatically adjusts the hearing aid gain to match the prescriptive targets for the individual hearing loss. Fitting rationales can be designed in an almost endless number of ways, depending on the specific goals you want to achieve for the patient. These goals might include:
- Maximum speech intelligibility
- Maximum comfort
- Maximum sound quality
- Immediate acceptance of hearing aid
- Maximum audibility across a broad range of frequencies
- Restoration of natural loudness perception
The majority of the large hearing aid manufacturing companies have developed a proprietary fitting rationale for their hearing devices rather than using a generic rationale, such as the National Acoustic Laboratory (NAL) or the Desired Sensation Level (DSL) rationales (Keidser, Brew, & Peck, 2003). What most fitting rationales have in common is that they attempt to balance a number of goals, which are often in conflict with one another, in the most optimal manner. For example, a patient might require a substantial amount of gain to obtain maximum speech intelligibility and audibility, but require a relatively modest amount of gain for comfort and immediate acceptance.
The ‘Widex Sound’ Fitting Rationale – Aiming for a Natural Sound Reproduction
The overall goals of the Widex fitting rationale are optimal speech understanding, natural sound quality, natural loudness reproduction, and preservation of comfort.
Optimal speech understanding in quiet and in noise
The Widex fitting rationale has optimal speech understanding in both quiet and noise as a primary fitting objective. Improved speech understanding in noise presents a challenge in connection with hearing-impaired listeners, as hearing loss is often accompanied by an increased sensitivity to masking effects and loss of both temporal and spectral resolution (i.e., a poorer ability to keep sounds that differ in terms of frequency content or time of occurrence perceptually apart) (Bernstein & Andrew, 2006; Florentine, Buus, & Scharf, 1980; Nelson & Freyman, 1987). Therefore, the hearing aid sound processing must be designed to compensate to the greatest extent possible for these effects.
A well-known phenomenon which may lead to reduced speech understanding in hearing aid users is masking. Masking occurs when a loud sound in one frequency region renders a sound in the same or another frequency region inaudible. A familiar example from everyday life needing to turn up the volume of your car radio to hear the news because it is being drowned by noise from the engine. This phenomenon of low-frequency noise (car noise in this example) drowning mid- or high-frequency sound (speech in this example) is referred to as upward spread of masking. Masking can also travel downwards in frequency, but this is much less pronounced than when it travels upwards. Moreover, since most noise sources are low in frequency, one focus of most hearing aid manufacturers is to prevent the upward spread of masking by trying to avoid excessive low-frequency gain.
Natural and transparent sound quality
Apart from providing the necessary amplification to ensure audibility and speech intelligibility, the goal is to offer a fully transparent sound quality. The sound reproduction should be as close to the original as possible, and the amplification of sound should not result in unintentional artifacts.
Moreover, we devote considerable effort to maintaining the balance between retaining the “fullness” of the natural sound to the widest extent possible by amplifying sound across a wide frequency spectrum, while at the same time minimizing the negative consequences of upward spread of masking through highly controlled application of low-frequency gain.
Natural loudness reproduction
Our goal at Widex is to amplify sound environments to a degree where they are perceived as natural as possible, consisting of soft, medium and loud sounds.
Soft sounds are a frequent and natural part of daily life. Our aim is to restore the audibility of as many of those sounds as possible. For some wearers, it will be difficult to get used to air conditioning, traffic outside the house, footsteps, et cetera, after having been deprived of these sounds for a long time. It is our experience that many wearers will get used to the presence of soft sounds and appreciate them in time. Care must be taken not to amplify them too much, though, so they become too dominant.
Medium sounds are typically at conversational input levels (60-70 dB SPL). The primary goal for these levels is to make speech intelligible while preserving comfort and naturalness. To do this, we generally follow the speech equalization principle, according to which normal speech shall be amplified to match the user’s MCL loudness contour (Byrne & Dillon, 1986).
Loud sounds should be loud, but not uncomfortably loud. In other words, they should be amplified to a degree where they are perceived as having the same loudness as they would be by a normal-hearing person. Again, care must be taken to ensure that loud sounds do not become unpleasantly loud, for instance, by implementing a controlled maximum output level of the hearing aid, and a feature which is capable of handling sudden, loud impulse sounds like a slamming door.
Preservation of comfort
Studies have shown that hearing-impaired individuals often have to work harder cognitively to process auditory information than normal-hearing individuals (Hetu, Riverin, Lalande, Getty, & St-Cyr, 1988; Hicks & Tharpe, 2002; Nachtegaal, Kuik, Anema, Goverts, Festen, et al., 2009). For example, Nachtegaal et al. (2009) found that hearing aid users had a greater self-reported need for recovery after work than normal-hearing workers. Similarly, a study by Hicks & Tharpe (2002) indicated that hearing impaired school-aged children expended a greater listening effort compared to their normal-hearing peers. Thus, for hearing aid users who rely on their hearing aids to lessen the impact of their hearing loss on their everyday lives, it is essential that the hearing aids do not raise the already increased listening effort further. An important fitting goal, therefore, is that the hearing aids are able to offer a sound quality that the wearer can listen to for many hours during the day without experiencing increased listening fatigue.
The overall goals of the Widex fitting rationale are summarized in Figure 3.

Figure 3. Summary of the overall goals of the Widex fitting rationale.
A Benchmark Test of the ‘Widex Sound Quality’
In order to systematically evaluate the ‘Widex Sound’, our latest wireless high-end device, the Widex DREAM440 hearing aid, was recently tested on a number of sound quality attributes alongside two high-end products from other leading manufacturers.
When testing sensory attributes, such as sound quality, it is important to keep in mind that specific physical attributes, such as the size of the hearing aid’s dynamic range, or the delay through the hearing aid, which we know affect hearing aid sound quality, are not necessarily meaningful, or even perceptually separable from other physical attributes for human listeners. The sound quality of the hearing aids were evaluated on a number of psychoacoustic attributes known to be correlated to human perception of hearing aid sound quality (Legarth, Simonsen, Dyrlund, Bramsløw, & Jespersen, 2012). The attributes included naturalness, fullness, distortion, tube sound, sharpness, and loudness. A definition of each attribute is available in Figure 4.
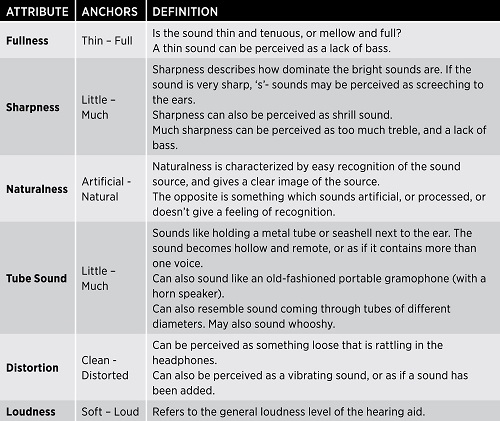
Figure 4. Anchors and definitions (translated from Danish) used to narrow down each attribute in the test.
To ensure impartiality, the test was conducted in a double-blinded study by a third party, the DELTA SenseLab in Denmark, using a panel of trained hearing impaired listeners as assessors. The panel had received training and familiarization in similar tasks prior to the trial. All three hearing aids were fitted to the moderately sloping N3 hearing loss of the IEC 60118-15 standard (Bisgaard, Vlaming, & Dahlquist, 2010). Recordings were made from each hearing aid in a number of environmental scenarios, including music, traffic, speech in quiet and speech in noise. The scenarios were selected to be representative for different hearing aid user environments. The sound quality of the hearing aids were evaluated on six different attributes known to be important for the perceived sound quality of a hearing aid (Legarth et al., 2012), using a continuous scale with an anchor label at each end such as this:
Example: Distortion Clean___________________________________________________Distorted
The main results of the benchmark test are shown as average ratings on each attribute in Figure 5.
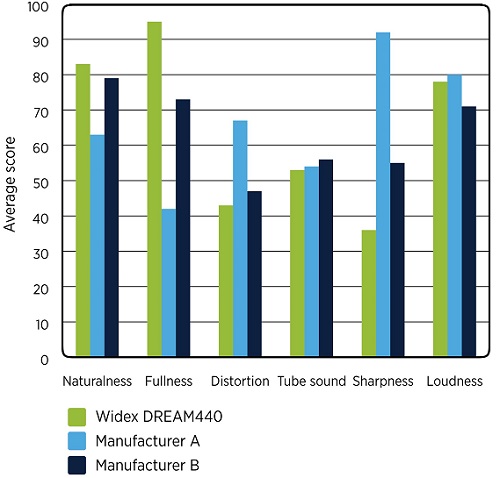
Figure 5. Evaluation of the Widex DREAM and two competing wireless premium products from leading manufacturers by a panel of hearing-impaired listeners.
We can see that the sound of the Widex DREAM440 is perceived as being characterized by a high degree of naturalness and fullness, a low degree of distortion, an average degree of tube sound, a low degree of sharpness, and medium loudness.
In comparison, the sound quality of the premium product from manufacturer A is characterized by a notably higher degree of sharpness and distortion, a similar degree of tube sound and loudness, and a notably lower degree of fullness and naturalness (Figure 5).
The sound quality of the premium product from manufacturer B is characterized by being notably sharper and less full than the sound quality of Widex DREAM440, and is also perceived to be slightly less natural, more distorted and softer than the Widex DREAM440 by the panel of hearing-impaired listeners (Figure 5).
The results from the independent trial suggest that we have succeeded in developing a hearing aid which is industry-leading in terms of offering a rich and well-balanced natural sound quality.
Conclusion
Evidence from large scale surveys (Kochkin, 2000; 2010) suggest that sound quality is a very important factor in relation to hearing aid satisfaction. From this perspective, the fitting of hearing aids with a high sound quality will clearly benefit both hearing care professionals and wearers. The increased satisfaction with the devices may lead to increased usage and acceptance among the patients, and ultimately to greater benefit from the hearing aids. Hearing care professionals will benefit from the increased user satisfaction by having fewer returns, less need for fine tuning, and fewer visits to the clinic. However, in order to develop products with a high sound quality, it is important to understand what constitutes a “good” sound quality in relation to a hearing impaired person.
One way to understand this is to review the available literature on what contributes to a good hearing aid sound quality. Using the existing evidence as the underlying basis, Widex has implemented the design parameters and fitting rationale which we believe provide the best sound quality for the wearer.
The total results of our efforts, which one might term ‘the Widex Sound’, was recently evaluated in an independent double-blinded trial conducted by a third party with a panel of trained hearing-impaired listeners acting as assessors. The results suggest that the Widex Sound is perceived to be well-balanced, very natural and full, and characterized by a low degree of distortion compared to the sound quality of two other high-end products from manufacturers considered to be leading when it comes to sound quality.
References
Bernstein, J. G., & Andrew, O. J. (2006). The relationship between frequency selectivity and pitch. Journal of the Acoustic Society of America, 120(6), 3929–3945.
Bisgaard, N., Vlaming, M. S. M. G., & Dahlquist, M (2010). Standard audiograms for the IEC 60118-15 measurement procedure. Trends in Amplification, 14(2) 113–120.
Boothroyd, A., & Medwetsky, L. (1992). Spectral distribution of /s/ and the frequency response of hearing aids. Ear and Hearing, 13(3), 150-157.
Byrne, D. & Dillon, H. (1986). The National Acoustic Laboratories’ (NAL) new procedure for selecting the gain and frequency response of a hearing aid. Ear and Hearing 7, 257-265
Chasin, M. (2003). Music and hearing aids. The Hearing Journal, 56, 7.
Chasin, M. (2007, February). Music as an input to a hearing aid. AudiologyOnline, Article 954. Retrieved from https://www.audiologyonline.com
Florentine, M., Buus, S., & Scharf, B. (1980). Frequency selectivity in normally-hearing and hearing-impaired observers. Journal of Speech and Hearing Research, 23, 646-669.
Gatehouse, S., Naylor, G., & Elberling, C. (2006). Linear and nonlinear hearing aid fittings: 1. Patterns of benefit. International Journal of Audiology, 45(3), 130-152.
Hansen, M. (2002). Effects of multi-channel compression time: constants on subjectively perceived sound quality and speech intelligibility. Ear and Hearing, 23(4), 369-380.
Hedrick, M., & Rice, T. (2000). Effect of a single-channel wide dynamic range compression circuit on perception of stop consonant place of articulation. Journal of Speech and Hearing Research, 43, 1174-1184.
Hetu, R., Riverin, L., Lalande, N., Getty, L., & St-Cyr, C. (1988). Qualitative analysis of the handicap associated with occupational hearing loss. British Journal of Audiology, 22(4), 251-264.
Hicks, C. B., & Tharpe, A. M. (2002). Listening effort and fatigue in school-age children with and without hearing loss. Journal of Speech, Language, and Hearing Research, 45(3), 573-584.
Jenstad, L. M., & Souza, P. E. (2005). Quantifying the effect of compression hearing aid release time on speech acoustics and intelligibility. Journal of Speech, Language, and Hearing Research, 48, 651-667.
Jongman, A., Wayland, R., & Wong, S. (2000). Acoustic characteristics of English fricatives. Journal of the Acoustical Society of America, 108(3), 1252-1263.
Keidser, G., Brew, C., & Peck, A. (2003). Proprietary fitting algorithms compared with one another and with generic formulas. The Hearing Journal, 56(3), 28-38.
Killion, M. C. (2009). What special hearing aid properties do performing musicians require? Hearing Review, 16(2), 20-31.
Kochkin, S. (2010). MarkeTrak VIII: Consumer satisfaction with hearing aids is slowly increasing. The Hearing Journal, 63(1), 19-32.
Kochkin, S. (2000). MarkeTrak V: “Why my hearing aids are in the drawer”: the consumer’s perspective. The Hearing Journal, 53(2), 34-41.
Legarth, S. V., Simonsen, C. S., Dyrlund, O., Bramsløw, L., & Jespersen, C. T. (2012, August). Establishing and qualifying a hearing impaired expert listener panel. Poster presented at the 2012 International Hearing Aid Research Conference (IHCON), Lake Tahoe, CA.
Moore, B. C. J., & Tan, C.-T. (2003). Perceived naturalness of spectrally distorted speech and music. Journal of the Acoustical Society of America, 114(1), 408-419.
Nachtegaal, J., Kuik, D. J., Anema, J. R., Goverts, S. T., Festen, J. M., & Kramer, S. E. (2009). Hearing status, need for recovery after work, and psychosocial work characteristics: Results from an internet-based national survey on hearing. International Journal of Audiology, 48(10), 684-691.
Nelson, D. A., & Freyman, R. L. (1987). Temporal resolution in sensorineural hearing-impaired listeners. Journal of the Acoustical Society of America, 81(3), 709-720.
Stelmachowicz, P. G., Lewis, D. E., Choi, S., & Hoover, B. (2007). Effect of stimulus bandwidth on auditory skills in normal-hearing and hearing impaired children. Ear and Hearing, 28, 483–494.
Stelmachowicz, P. G., Pittman, A. L., Hoover, B. M., & Lewis, D. E. (2001). Effect of stimulus bandwidth on the perception of /s/ in normal and hearing-impaired children and adults. Journal of the Acoustical Society of America, 110, 2183– 2190.
Stone, M. A., & Moore, B. C. (1999). Tolerable hearing aid delays. I. Estimation of limits imposed by auditory path alone using simulated hearing losses. Ear and Hearing 20(3), 182-192.
Stone, M. A., & Moore, B. C. (2003). Tolerable hearing aid delays. III. Effects on speech production and perception of across-frequency variation in delay. Ear and Hearing 24(2), 175-183.
Todd, A. E., Edwards, J. R., & Litovsky, R., Y. (2011). Production of contrast between sibilant fricatives by children with cochlear implants. Journal of the Acoustical Society of America, 130(6), 3969-3979.
Whitmer, W. M., Brennan-Jones, C. G, & Akeroyd, M. A. (2011). The speech intelligibility benefit of a unilateral wireless system for hearing-impaired adults. International Journal of Audiology, 50(12), 905-911.
Yavas, M. (2006). Applied English phonology. Malden, MA: Blackwell Publishing.
Cite this content as:
Jessen, A.H., Baekgaard, L., & Andersen, H. P. (2014, January). What is good hearing aid sound quality, and does it really matter? AudiologyOnline, Article 12340. Retrieved from: https://www.audiologyonline.com



